
Considering trenbolone? The side effects are worse than almost any other steroid. Here’s what actually happens, ranked by severity.
You hear trenbolone is the most powerful steroid. You see the transformation photos. You want those results.
But you don’t fully understand what you’re signing up for. Trenbolone’s side effect profile is among the worst in the entire steroid category.
You’ve been told:
- “Side effects are manageable with proper protocols”
- “Only happens to careless users”
- “The gains are worth it”
- “You can control everything with ancillaries”
Much of this is dangerously optimistic. The truth: Trenbolone causes side effects that range from cosmetic annoyances (acne, hair loss) to serious health threats (cardiovascular damage, severe insomnia, psychological disorders). Some effects are preventable or reversible. Many are not. Genetics, dosage, and duration influence severity, but trenbolone is harsher than most steroids regardless. Understanding each side effect likelihood, preventability, reversibility, and health risk is essential before first injection.
In this comprehensive guide, I’ll rank 9 trenbolone side effects by health risk (low to high severity), reveal likelihood and preventability for each (realistic expectations), explain the mechanisms (why they occur), provide reversal potential (what’s permanent vs. temporary), and compare to other steroids (trenbolone’s unique harshness).
Whether you’re considering trenbolone or currently using it, understanding these risks is critical.
Let’s examine trenbolone’s side effect profile scientifically and honestly.
TABLE OF CONTENTS
Understanding the Side Effect Categories
The framework for analysis.
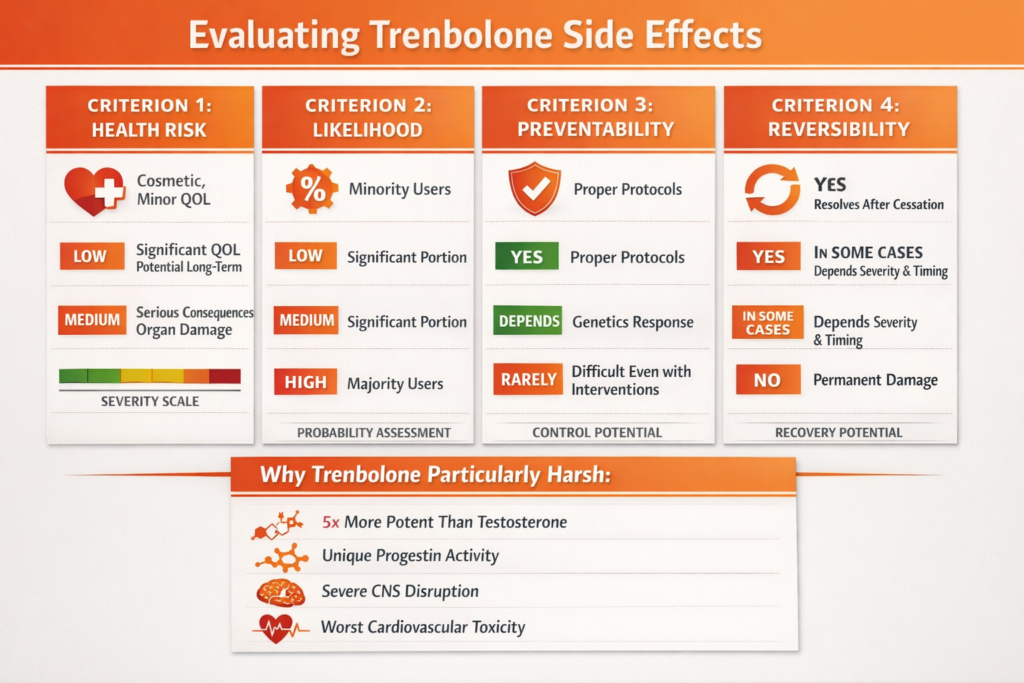
The Four Evaluation Criteria
For each side effect, we assess:
1. Health risk:
- Low: Cosmetic or minor quality of life impact
- Medium: Significant quality of life impact or potential long-term issues
- High: Serious health consequences, organ damage risk
- Severity scale
2. Likelihood:
- Low: Affects minority of users
- Medium: Affects significant portion of users
- High: Affects majority of users
- Probability
3. Preventability:
- Yes: Can be avoided with proper protocols
- Depends: Based on individual genetics/response
- Rarely: Difficult to prevent even with interventions
- No: Unavoidable with trenbolone use
- Control potential
4. Reversibility:
- Yes: Resolves after cessation
- In some cases: Depends on severity and intervention timing
- No: Permanent damage
- Recovery potential
Why Trenbolone Is Particularly Harsh
The potency factor:
- Trenbolone is 5x more anabolic than testosterone
- Also 5x more androgenic
- Extremely potent = extreme effects (good and bad)
- Power and consequences
No aromatization BUT progestin activity:
- Doesn’t convert to estrogen (positive)
- BUT has progestogenic effects (problematic)
- Elevates prolactin (indirect estrogen-like effects)
- Unique hormonal profile
Neurological impact:
- Particularly harsh on nervous system
- More psychological side effects than most steroids
- CNS disruption
Cardiovascular toxicity:
- One of worst steroids for lipid profile
- Direct cardiotoxic effects
- Heart and vascular damage
The comparison:
- Testosterone: Moderate side effects, mostly manageable
- Nandrolone: Moderate, some similar to tren but less severe
- Trenbolone: Severe across multiple categories
- Worst profile
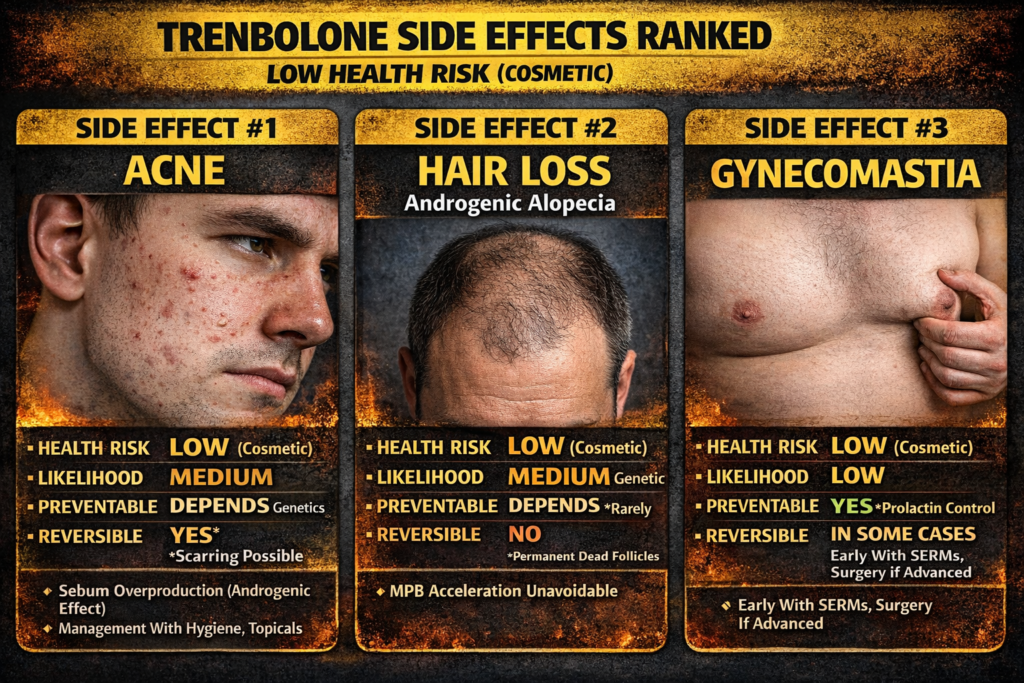
Side Effect 1: Acne
Health Risk: LOW | Likelihood: MEDIUM | Preventable: DEPENDS | Reversible: YES
The Mechanism
Why trenbolone causes acne:
- Extremely androgenic (5x testosterone)
- Stimulates sebaceous glands
- Increases sebum (oil) production
- Androgenic effect on skin
The process:
- More androgens = more sebum
- Excess sebum clogs pores
- Bacteria (P. acnes) proliferate
- Inflammation and acne form
- Acne development
Individual variation:
- People prone to acne affected most
- Clean skin individuals may avoid it
- Genetics determine susceptibility
- Personal predisposition
Likelihood and Severity
Who gets it:
- History of acne: High likelihood
- Oily skin naturally: Medium-high likelihood
- Clear skin history: Low-medium likelihood
- Risk factors
Where it appears:
- Face (most noticeable)
- Back (“bacne” common)
- Shoulders and chest
- Distribution
The severity:
- Ranges from mild breakouts to severe cystic acne
- Dose-dependent (higher dose = worse)
- Variable intensity
Prevention and Management
Can you prevent it:
- Partially, depends on genetics
- Limited control
Prevention strategies:
Hygiene:
- Shower immediately after training
- Wash face twice daily
- Change pillowcases frequently
- Cleanliness
Topical treatments:
- Benzoyl peroxide
- Salicylic acid
- Retinoids (prescription)
- OTC and prescription options
Oral medications (severe cases):
- Antibiotics (doxycycline, minocycline)
- Isotretinoin (Accutane) for severe cases
- Medical intervention
The reality:
- Even with perfect hygiene, some people get acne
- Trenbolone is particularly harsh
- Management possible but not always prevention
- Genetic lottery
Reversibility
After stopping trenbolone:
- Acne typically resolves within weeks to months
- Sebum production normalizes
- Breakouts cease
- Temporary problem
Scarring risk:
- Severe cystic acne can leave permanent scars
- Early treatment prevents scarring
- Potential permanent cosmetic damage
The verdict:
- Acne itself reverses
- Scars may be permanent
- Mostly reversible
Side Effect 2: Hair Loss (Androgenic Alopecia)
Health Risk: LOW | Likelihood: MEDIUM | Preventable: DEPENDS | Reversible: NO
The Mechanism
Why trenbolone causes hair loss:
- Trenbolone is NOT a DHT derivative
- Does NOT convert to DHT
- BUT binds strongly to androgen receptors in scalp
- Direct androgenic effect
The process:
- Androgens bind to scalp follicle receptors
- Miniaturize hair follicles
- Hairs become thinner and shorter
- Eventually, follicles die
- Progressive follicle destruction
The genetic factor:
- Male pattern baldness (MPB) genes required
- If genetically prone: High risk
- If no MPB genetics: Lower risk (but not zero)
- Genetic predisposition essential
Likelihood and Severity
Who’s at risk:
- Family history of baldness: Very high risk
- Already thinning: Accelerated loss certain
- Full head of hair with no family history: Lower risk
- Genetic determination
The pattern:
- Follows MPB pattern (temples, crown)
- Accelerated version of genetic destiny
- Happens much faster than natural baldness
- Rapid progression
Prevention Attempts (Mostly Ineffective)
Why typical hair loss drugs don’t work:
Finasteride/Dutasteride (5α-reductase inhibitors):
- Block conversion of testosterone to DHT
- Trenbolone doesn’t convert to DHT
- Completely ineffective for trenbolone
The futility:
- No effective prevention exists
- Can’t block trenbolone from binding receptors
- Unavoidable if genetically prone
What some try (limited effectiveness):
- RU58841 (topical anti-androgen, experimental)
- Minoxidil (promotes growth but doesn’t prevent loss)
- Ketoconazole shampoo (marginal benefit)
- Desperation measures
The reality:
- If you’re genetically prone, trenbolone will cause hair loss
- No reliable prevention
- Accept or avoid trenbolone
Reversibility
The harsh truth:
- Dead follicles don’t come back
- Hair loss from trenbolone is permanent
- Irreversible
Stopping progression:
- Discontinuing trenbolone stops further loss
- But lost hair stays lost
- Damage done is done
Hair transplant option:
- Can surgically relocate follicles
- Expensive ($5,000-$15,000+)
- Doesn’t prevent future loss
- Cosmetic fix only
Side Effect 3: Gynecomastia (Gyno)
Health Risk: LOW | Likelihood: LOW | Preventable: YES | Reversible: IN SOME CASES
The Mechanism
The estrogen paradox:
- Trenbolone does NOT aromatize (convert to estrogen)
- Does NOT directly increase estrogen
- So why gyno?
The prolactin pathway:
- Trenbolone has progestogenic activity
- Increases prolactin levels
- Elevated prolactin increases estrogen sensitivity
- Breast tissue responds to normal estrogen levels as if elevated
- Indirect estrogenic effect
The binding:
- Progesterone can bind to progesterone receptors in breast tissue
- Contributes to gyno development
- Progestin contribution
Likelihood and Severity
Probability:
- Lower than with aromatizing steroids (testosterone, dianabol)
- But still possible
- Dose and individual sensitivity determine risk
- Medium-low occurrence
Risk factors:
- Using trenbolone with aromatizing compounds (stacked cycles)
- High doses
- Long duration
- Personal sensitivity
- Compounding factors
Prevention
Can be prevented:
- More controllable than with aromatizing steroids
- Yes, manageable
Prevention strategies:
Prolactin control:
- Cabergoline (dopamine agonist, lowers prolactin)
- 0.25-0.5mg twice weekly
- Most effective prevention
- Prolactin management
Estrogen control (if stacking):
- If using with aromatizing compounds
- AI (anastrozole, exemestane)
- Controls estrogen from other compounds
- Stack-dependent
SERMs (if early signs):
- Nolvadex or raloxifene
- Blocks estrogen at breast tissue
- Can reverse early gyno
- Receptor blocking
Monitoring:
- Check for lumps under nipples weekly
- Sensitivity or puffiness = early warning
- Act immediately if noticed
- Early detection
Reversibility
Early-stage gyno:
- Small lumps (<1cm)
- Caught within weeks of development
- Reversible with SERMs (nolvadex, raloxifene)
- 60-80% success rate if treated early
- Potentially reversible
Established gyno:
- Large lumps (>1cm)
- Present for months
- Glandular tissue fully formed
- Surgery only option (gynecomastia surgery, $4,000-$8,000)
- Irreversible without surgery
The verdict:
- Preventable with prolactin control
- Reversible if caught early
- Surgery required if advanced
- Time-sensitive
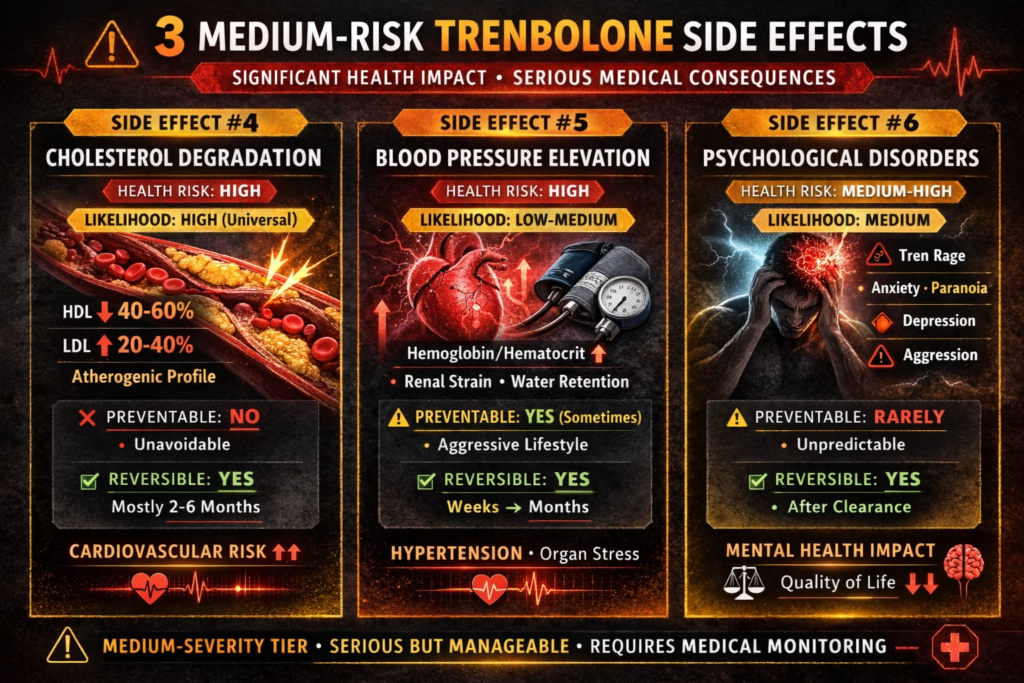
Side Effect 4: Cholesterol Degradation
Health Risk: HIGH | Likelihood: HIGH | Preventable: NO | Reversible: YES (mostly)
The Mechanism
How all steroids affect cholesterol:
- Steroids alter liver enzyme function
- Specifically affect: Hepatic lipase and lipoprotein lipase
- Results in HDL degradation and LDL accumulation
- Hepatic metabolism disruption
Why trenbolone is particularly bad:
- Extremely androgenic (5x testosterone)
- More androgenic = worse lipid effects
- Trenbolone among worst steroids for cholesterol
- Severity factor
The numbers:
- HDL (good cholesterol): Drops 40-60%
- LDL (bad cholesterol): Increases 20-40%
- Total cholesterol ratio severely unfavorable
- Dramatic shift
Likelihood and Severity
Probability:
- Occurs in virtually all users
- Degree varies but always present
- Universal effect
Severity spectrum:
- Mild use (200mg/week): Moderate impact
- Heavy use (400mg+/week): Severe impact
- Dose-dependent
The cardiovascular risk:
- Atherogenic profile (promotes plaque formation)
- Increased heart attack and stroke risk
- Accelerated atherosclerosis
- Serious health threat
Prevention Attempts (Limited Effectiveness)
Can you prevent it:
- No, cholesterol disruption unavoidable
- Can only minimize severity
- Inevitable
Damage control strategies:
Diet optimization:
- High fiber (oats, vegetables, beans)
- Omega-3 fatty acids (fish, fish oil)
- Minimize saturated fats
- Avoid trans fats
- Dietary intervention
Cardiovascular exercise:
- 150+ minutes moderate cardio weekly
- Improves HDL slightly
- Reduces LDL slightly
- Can’t fully counteract trenbolone’s effects
- Aerobic work
Supplements:
- Fish oil (2-4g daily)
- Niacin (controversial, liver stress)
- Plant sterols
- Coenzyme Q10
- Marginal benefits
The reality:
- Even with perfect diet and cardio, lipids still worsen
- Only minimizes damage, doesn’t prevent
- Mitigation not prevention
Reversibility
After discontinuation:
- Cholesterol begins improving within weeks
- Normalization: 2-6 months typically
- Full recovery possible if no permanent vascular damage
- Gradual recovery
The timeline:
- Month 1: Slight improvement
- Month 2-3: Significant improvement
- Month 4-6: Near or complete normalization
- Months-long process
The permanent damage question:
- Cholesterol levels reverse
- BUT: Atherosclerotic plaques formed during use may not fully regress
- Arterial damage can be permanent
- Cholesterol reverses, vascular damage may not
The risk:
- Longer duration = more plaque formation
- Higher doses = more damage
- Multiple cycles = cumulative risk
- Time and dose dependent
Side Effect 5: Elevated Blood Pressure
Health Risk: HIGH | Likelihood: LOW-MEDIUM | Preventable: YES (sometimes) | Reversible: YES
The Mechanism
How trenbolone raises blood pressure:
Mechanism 1: Increased hematocrit
- Trenbolone stimulates red blood cell production
- More RBCs = thicker blood
- Thicker blood = higher pressure
- Blood viscosity
Mechanism 2: Renal effects
- Affects kidney function
- Alters sodium retention
- Increases blood volume
- Kidney pathway
Mechanism 3: Arterial stiffness
- Cholesterol changes affect arterial compliance
- Stiffer arteries = higher pressure
- Vascular changes
Likelihood and Severity
Probability:
- Lower than cholesterol disruption
- But significant portion of users affected
- Pre-existing hypertension = much higher risk
- Medium occurrence
Risk factors:
- Already have high blood pressure: Very high risk (contraindicated)
- Salt-sensitive: Higher risk
- Poor diet: Higher risk
- Sedentary: Higher risk
- Individual factors
The numbers:
- Can increase systolic 10-20+ mmHg
- Diastolic 5-15+ mmHg
- Some users exceed 140/90 (hypertensive)
- Significant elevation
Prevention and Management
Can be prevented:
- Sometimes, with aggressive lifestyle measures
- Not always
- Partial control
Prevention strategies:
Dietary sodium restriction:
- <2,000mg sodium daily
- Reduces blood volume
- Meaningful impact
- Salt reduction
Potassium increase:
- 3,500-5,000mg daily
- Counters sodium effects
- From food or supplements
- Electrolyte balance
Cardiovascular exercise:
- 150+ minutes weekly
- Lowers resting blood pressure
- Essential, not optional
- Aerobic necessity
Hydration:
- Adequate water intake
- Supports kidney function
- Fluid balance
Medications (if needed):
- ARBs (losartan, telmisartan)
- ACE inhibitors
- Beta-blockers (can hurt gym performance)
- Medical supervision required
- Pharmaceutical control
Monitoring:
- Check blood pressure 2-3x weekly minimum
- Home blood pressure monitor
- Track trends
- Regular assessment
Reversibility
After cessation:
- Blood pressure typically normalizes
- Timeline: Weeks to months
- Faster than cholesterol recovery
- Reversible
The chronic risk:
- Prolonged hypertension damages arteries
- Can become chronic condition
- Kidney damage risk
- Heart remodeling risk
- Potential permanent consequences
The verdict:
- Blood pressure itself reverses
- But damage during hypertensive periods may be permanent
- Mostly reversible if caught early
Side Effect 6: Psychological Disorders
Health Risk: MEDIUM-HIGH | Likelihood: MEDIUM | Preventable: RARELY | Reversible: YES
The Mechanism
How trenbolone affects the brain:
- Brain has androgen receptors
- Physiological testosterone levels = normal brain function
- Supraphysiological androgens = disrupted neurotransmitters
- Neurochemical imbalance
The neurotransmitter disruption:
- Dopamine dysregulation
- Serotonin imbalance
- GABA disruption
- Multiple systems affected
Trenbolone’s unique harshness:
- More potent than most steroids
- Stronger binding to brain receptors
- More severe psychological effects
- Neurological severity
The Psychological Effects
Common manifestations:
“Tren rage” (aggression):
- Increased irritability
- Short temper
- Disproportionate anger responses
- Violence potential (in some users)
- Aggression escalation
Anxiety:
- Generalized anxiety
- Social anxiety
- Panic attacks (in some)
- Anxious state
Paranoia:
- Unfounded suspicions
- Relationship distrust
- Persecution feelings
- Paranoid thinking
Depression:
- Low mood
- Anhedonia (inability to feel pleasure)
- Hopelessness
- Depressive symptoms
Mood swings:
- Rapid emotional shifts
- Unpredictable reactions
- Emotional instability
- Lability
Likelihood and Severity
Probability:
- Affects significant portion of users
- Severity varies widely
- Dose-dependent
- Medium-high occurrence
Risk factors:
- History of mental health issues: Much higher risk
- High doses: Higher risk
- Stressful life circumstances: Amplified
- Vulnerability factors
The spectrum:
- Mild: Slightly increased irritability (manageable)
- Moderate: Noticeable personality changes (concerning)
- Severe: Relationship destruction, violence, suicidal ideation (dangerous)
- Wide range
Prevention
Can you prevent it:
- Rarely
- Very difficult to predict who will be affected
- Limited control
Mitigation attempts:
Lower doses:
- Less trenbolone = less neurological impact
- But still no guarantee
- Dose reduction
Avoid stacking with other harsh compounds:
- Trenbolone alone is harsh enough
- Multiple compounds amplify effects
- Simplification
Stress management:
- Meditation, therapy
- Reduces baseline stress
- May slightly buffer effects
- Lifestyle factors
The reality:
- Even low doses cause psychological issues in some people
- Unpredictable individual response
- Genetic lottery
Reversibility
After discontinuation:
- Psychological symptoms resolve as trenbolone clears
- Timeline: Weeks to months (depending on ester)
- Full recovery expected in most cases
- Temporary
The clearance timeline:
- Trenbolone acetate: 2-4 weeks for significant improvement
- Trenbolone enanthate: 4-8 weeks
- Ester-dependent
Long-term effects:
- No evidence of permanent brain damage from trenbolone alone
- But severe episodes can have lasting psychological impact (trauma from behavior, relationship damage)
- Behavioral consequences may outlast chemical effects
The verdict:
- Chemical effects reverse
- Life consequences of behavior may be permanent
- Chemically reversible, situationally complicated
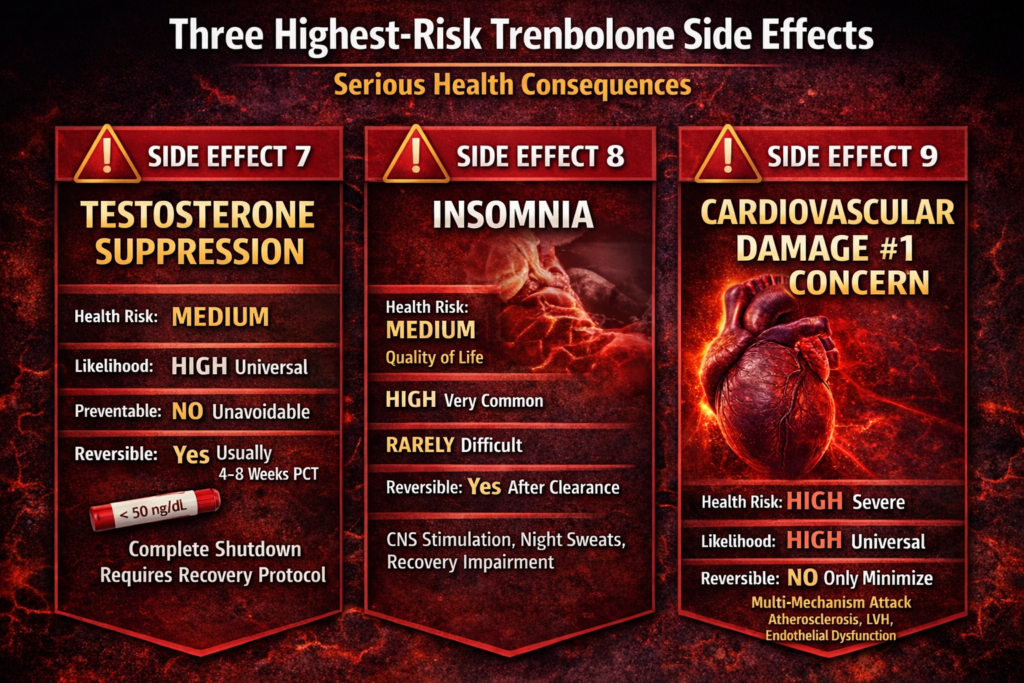
Side Effect 7: Testosterone Suppression
Health Risk: MEDIUM | Likelihood: HIGH | Preventable: NO | Reversible: YES (usually)
The Mechanism
How trenbolone shuts down natural testosterone:
- Hypothalamic-pituitary-testicular (HPT) axis feedback
- Brain detects high androgen levels
- Signals testes to stop producing testosterone
- Negative feedback loop
The speed and severity:
- Trenbolone extremely suppressive
- Shutdown occurs within days
- Near-complete suppression common
- Rapid and total
The comparison:
- Testosterone: Suppressive but gradual
- Trenbolone: Suppressive and immediate
- Faster shutdown
Likelihood and Severity
Probability:
- Occurs in all users without exception
- Complete shutdown in majority
- Universal effect
The numbers:
- Natural testosterone: 300-1000 ng/dL (normal range)
- On trenbolone: <50 ng/dL (severely suppressed)
- Dramatic suppression
Why This Matters
The symptoms of low testosterone (post-cycle):
- Fatigue and low energy
- Depression
- Loss of libido
- Erectile dysfunction
- Muscle loss
- Fat gain
- Hypogonadal symptoms
The timing:
- During cycle: Trenbolone replaces testosterone (symptoms masked)
- Post-cycle: Trenbolone declining, testosterone still shut down (crash)
- The crash period
Prevention
Can you prevent suppression:
- No, unavoidable with trenbolone use
- Inevitable
Managing during cycle:
- Include testosterone in cycle (most people do)
- Provides exogenous testosterone
- Prevents low-T symptoms during cycle
- Testosterone base
The standard protocol:
- Trenbolone + testosterone base (200-500mg/week)
- Maintains physiological testosterone levels
- Stacking necessity
Reversibility (Post-Cycle Therapy)
Natural recovery:
- Without intervention: 6-12 months for natural recovery
- Symptoms severe during recovery
- Muscle loss significant
- Slow natural recovery
With PCT (Post-Cycle Therapy):
- SERMs (Clomid, Nolvadex)
- Stimulate LH and FSH production
- Restart testicular testosterone production
- Faster recovery: 4-8 weeks
- Accelerated recovery
Standard PCT protocol:
- Wait for trenbolone to clear (ester-dependent)
- Clomid 50mg daily + Nolvadex 20mg daily for 4-6 weeks
- Or variations
- Recovery protocol
Success rate:
- Most people recover fully
- Some experience prolonged suppression (months to year+)
- Rare cases: Permanent hypogonadism (require TRT for life)
- Usually reversible
Risk factors for poor recovery:
- Long cycles (>12 weeks)
- Multiple cycles without adequate breaks
- High doses
- Age (older = slower recovery)
- Cumulative factors
Side Effect 8: Insomnia
Health Risk: MEDIUM | Likelihood: HIGH | Preventable: RARELY | Reversible: YES
The Mechanism
How trenbolone disrupts sleep:
- CNS stimulation (central nervous system activation)
- Neurotransmitter disruption (dopamine, serotonin)
- Maintains brain in alert state
- Prevents relaxation necessary for sleep
- Neurological arousal
The specific effects:
- Difficulty falling asleep
- Frequent night awakenings
- Early morning waking
- Non-restorative sleep
- Multiple sleep disruptions
Night sweats (related):
- Trenbolone affects thermoregulation
- Profuse sweating during sleep
- Wakes user up
- Compounds insomnia
- Temperature dysregulation
Likelihood and Severity
Probability:
- One of most commonly reported side effects
- Affects majority of users
- Very common
The severity spectrum:
- Mild: Slight sleep difficulty (5-6 hours instead of 8)
- Moderate: Significant sleep disruption (4-5 hours, fragmented)
- Severe: Chronic severe insomnia (2-3 hours, completely disrupted)
- Wide range
Dose relationship:
- Higher doses = worse insomnia
- But even low doses cause issues in many people
- Dose-dependent but pervasive
Prevention
Can you prevent it:
- Very difficult without pharmaceutical intervention
- Rarely
Non-pharmaceutical attempts (limited success):
- Sleep hygiene (cool room, dark, no screens)
- Melatonin (may help slightly)
- Magnesium (before bed)
- Glycine (3-5g before bed)
- Marginal benefits
Pharmaceutical options:
- Sleep medications (zolpidem, eszopiclone)
- Benzodiazepines (not recommended long-term)
- Antihistamines (diphenhydramine)
- Additional drugs required
The problem with sleep meds:
- Adds another layer of side effects
- Dependency risk
- May not fully resolve trenbolone-induced insomnia
- Complication
The Impact
Why insomnia is a serious problem:
Recovery impairment:
- Muscle repair occurs during sleep
- Poor sleep = poor recovery
- Counteracts training gains
- Performance sabotage
Health consequences:
- Chronic sleep deprivation increases cortisol
- Weakens immune system
- Impairs cognitive function
- Increases injury risk
- Multiple health impacts
Quality of life:
- Persistent fatigue
- Mood disruption (compounds psychological effects)
- Relationship strain
- Life quality degradation
The irony:
- Using trenbolone to optimize physique
- But insomnia undermines recovery and results
- Counterproductive
Reversibility
After discontinuation:
- Insomnia resolves as trenbolone clears
- Sleep normalizes within weeks
- Temporary
The timeline:
- Trenbolone acetate: 1-2 weeks improvement
- Trenbolone enanthate: 3-4 weeks improvement
- Ester-dependent
The verdict:
- Completely reversible
- No permanent sleep damage
- Full recovery expected
Side Effect 9: Cardiovascular System Damage
Health Risk: HIGH | Likelihood: HIGH | Preventable: NO | Reversible: PARTIALLY
The Multi-Faceted Attack
Why cardiovascular damage is #1 concern:
- Trenbolone harms cardiovascular system through multiple mechanisms simultaneously
- Cumulative effect worse than any single pathway
- Multi-system assault
The mechanisms:
1. Severe lipid profile disruption:
- HDL drops 40-60% (removes protective cholesterol)
- LDL increases 20-40% (accumulates plaque)
- Promotes atherosclerosis
- Atherogenic profile
2. Elevated blood pressure:
- Chronic hypertension damages arterial walls
- Increases cardiac workload
- Arterial stiffening
- Hypertensive damage
3. Direct cardiotoxicity:
- Trenbolone may directly damage heart muscle cells
- Left ventricular hypertrophy (heart thickening)
- Reduced cardiac efficiency
- Myocardial effects
4. Increased hematocrit:
- Thicker blood strains heart
- Increases clotting risk
- Blood viscosity
5. Endothelial dysfunction:
- Damage to arterial lining
- Impairs vasodilation
- Increases inflammation
- Vascular endothelium damage
Likelihood and Severity
Probability:
- Cardiovascular stress occurs in all users
- Severity varies but always present
- Universal impact
The progression:
- Acute: Immediate lipid changes, potential BP elevation
- Chronic: Progressive arterial damage, cardiac remodeling
- Long-term: Atherosclerotic disease, heart failure risk
- Time-dependent deterioration
Risk factors:
- Pre-existing cardiovascular disease: Extremely high risk (absolutely contraindicated)
- Family history of heart disease: Higher risk
- Poor lifestyle (smoking, bad diet, no cardio): Amplified risk
- Age (older = more vulnerable)
- Vulnerability factors
Prevention
Can you prevent cardiovascular damage:
- No, some degree of damage unavoidable
- Can only minimize severity
- Inevitable harm
Damage minimization strategies:
Cardiovascular exercise (mandatory):
- 150+ minutes moderate cardio weekly minimum
- More is better
- Not optional, essential for survival
- Aerobic necessity
Optimal nutrition:
- Anti-inflammatory diet
- High fiber
- Omega-3 fatty acids
- Antioxidant-rich foods
- Dietary intervention
Blood pressure management:
- Monitor regularly
- Medicate if needed (ARBs preferred)
- Keep <140/90
- BP control
Lipid management attempts:
- Diet and cardio (marginal benefit)
- Statins (controversial during cycle)
- Limited options
Avoid other cardiac stressors:
- Don’t smoke
- Limit alcohol
- Manage stress
- Lifestyle optimization
The reality:
- Even perfect protocols only minimize damage
- Cannot eliminate cardiovascular stress
- Mitigation not prevention
Reversibility
What reverses after stopping:
- Lipid profile: Normalizes over 2-6 months (mostly)
- Blood pressure: Normalizes over weeks to months (usually)
- Hematocrit: Returns to normal within weeks
- Some parameters recover
What may not reverse:
- Atherosclerotic plaques: May partially regress but often permanent
- Arterial stiffness: Partially reverses but some damage permanent
- Left ventricular hypertrophy: May partially regress, sometimes permanent
- Endothelial damage: Partially recovers
- Structural damage often permanent
The cumulative effect:
- One cycle: Some recovery possible
- Multiple cycles: More permanent damage
- Years of use: Significant irreversible damage likely
- Dose and duration dependent
The long-term prognosis:
- Increased heart attack risk (even years after cessation)
- Increased stroke risk
- Premature cardiovascular disease
- Potential heart failure
- Lasting consequences
The verdict:
- Functional parameters reverse (lipids, BP)
- Structural damage partially or not reversible
- Long-term cardiovascular risk elevated permanently
- Partially reversible at best
The Bottom Line: The Trenbolone Risk Profile
Ranking by health risk (low to high):
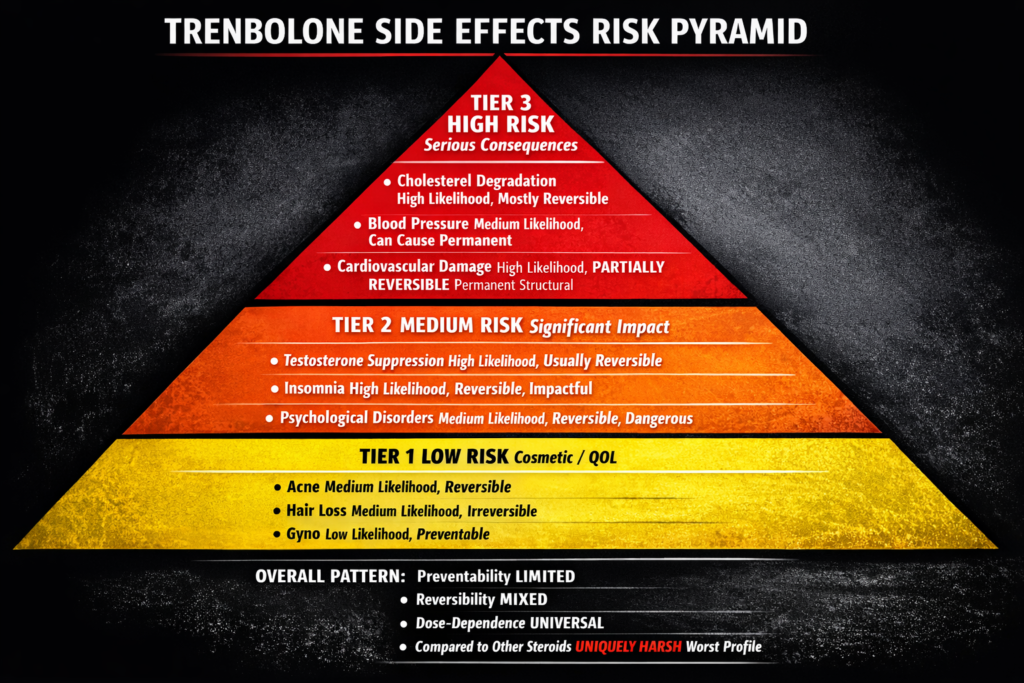
Low risk (cosmetic/quality of life):
- Acne (medium likelihood, reversible)
- Hair loss (medium likelihood, irreversible)
- Gynecomastia (low likelihood, preventable/reversible if early)
Medium risk (significant health impact): 4. Testosterone suppression (high likelihood, usually reversible) 5. Insomnia (high likelihood, reversible but impactful) 6. Psychological disorders (medium likelihood, reversible but potentially dangerous)
High risk (serious health consequences): 7. Cholesterol degradation (high likelihood, mostly reversible) 8. Blood pressure elevation (medium likelihood, reversible but can cause permanent damage) 9. Cardiovascular system damage (high likelihood, partially reversible)
The overall pattern:
- Cosmetic issues: Manageable but concerning
- Hormonal issues: Significant but recoverable
- Cardiovascular issues: Serious and partially permanent
- Progressive severity
Preventability summary:
- Preventable: Gyno (with prolactin control)
- Sometimes preventable: Blood pressure (with aggressive management)
- Depends on genetics: Acne, hair loss
- Rarely preventable: Psychological issues, insomnia
- Unavoidable: Cholesterol degradation, testosterone suppression, cardiovascular stress
- Limited control overall
Reversibility summary:
- Fully reversible: Acne, insomnia, testosterone suppression (usually), psychological effects, blood pressure
- Partially reversible: Gyno (if early), cardiovascular damage
- Irreversible: Hair loss, advanced gyno, some cardiovascular structural changes
- Mixed outcomes
The dose-dependence:
- All side effects worse at higher doses
- But even “low” doses (200mg/week) cause significant issues
- No “safe” dose exists
- Universal dose-response
The trenbolone paradox:
- Most powerful steroid for muscle gain
- Also worst side effect profile
- Risk-benefit calculation highly unfavorable
- Power comes with severe price
Compared to other steroids:
- Testosterone: Moderate sides, mostly manageable
- Nandrolone: Moderate sides, somewhat similar to tren but less severe
- Dianabol: Harsh but less harsh than tren
- Trenbolone: Worst overall profile
- Uniquely harsh
The informed decision:
- If using trenbolone, understand consequences
- Many effects unavoidable regardless of precautions
- Some damage potentially permanent
- Frequent monitoring essential
- Accept risks or avoid compound
This article is informational only. We do not condone or recommend steroid use. If considering any hormone therapy, work with qualified medical professionals and understand the serious health risks involved.
REFERENCES
SECTION 1 — Side Effect 1: Acne (Androgenic Mechanism)
[1] Melnik B et al. — Journal of the German Society of Dermatology, 2007 Abuse of anabolic-androgenic steroids and bodybuilding acne: an underestimated health problem — AAS enlarge sebaceous glands increasing sebum production; androgen receptors found in sebocytes and follicular keratinocytes; supraphysiological androgens increase C. acnes proliferation; acne reported in ~43-50% of AAS users; acne fulminans (severe hemorrhagic form) documented in bodybuilders; permanent scarring possible https://pubmed.ncbi.nlm.nih.gov/17274777/
[2] Habeshian KA & Cohen BA — PMC/Dermatology, 2020 Cutaneous Manifestations of Anabolic-Androgenic Steroid Use in Bodybuilders — comprehensive review of AAS dermatological side effects; acne mechanism via sebaceous gland enlargement and sebum overproduction; dose-dependent relationship confirmed; AAS-specific acne appears on face, back, shoulders and chest; severity ranges from mild breakouts to severe cystic acne; early isotretinoin intervention recommended for severe cases https://pmc.ncbi.nlm.nih.gov/articles/PMC10436113/
SECTION 2 — Side Effect 2: Hair Loss (Androgenic Alopecia)
[3] Kaufman KD et al. (Finasteride Male Pattern Hair Loss Study Group) — Journal of the American Academy of Dermatology, 1998 Finasteride in the treatment of men with androgenetic alopecia — androgenic alopecia caused by androgen-dependent follicle miniaturization; finasteride works by blocking conversion of testosterone to DHT via 5α-reductase inhibition; mechanism confirms hair loss requires DHT or direct androgen receptor activation at scalp; compounds not requiring 5α-reduction (such as trenbolone) bypass finasteride’s mechanism of action entirely; established genetic predisposition as essential factor https://pubmed.ncbi.nlm.nih.gov/9777765/
[4] Randall VA — Clinical Endocrinology, 2008 Androgens and hair growth — androgens regulate hair follicle cycling via androgen receptors in dermal papillae; follicle miniaturization occurs through direct androgen receptor binding independent of DHT conversion; 5α-reductase inhibitors ineffective for compounds binding androgen receptors directly without DHT conversion; genetic predisposition determines scalp follicle sensitivity; dead follicles do not regenerate https://pubmed.ncbi.nlm.nih.gov/18315727/
SECTION 3 — Side Effect 3: Gynecomastia (Prolactin/Progestin Pathway)
[5] Trenbolone Acetate — Wikipedia / Primary Source: Pharmacological Profile Trenbolone acetate pharmacological profile — confirmed agonist of progesterone receptor (PR) with moderate-to-strong progestogenic activity; does not aromatize to estrogen; progestogenic activity at breast tissue progesterone receptors contributes to gynecomastia; gyno possible despite absent estrogenic activity; dopamine agonists (cabergoline) recommended to control prolactin-mediated pathway https://en.wikipedia.org/wiki/Trenbolone_acetate
[6] Petersenn S et al. — PMC / Endocrinology, 2023 Cabergoline treatment in men with microprolactinoma — cabergoline (dopamine agonist) normalizes prolactin in 89.4% of hyperprolactinemic men; mechanism: dopamine agonism at pituitary inhibits prolactin secretion; testosterone and gonadal axis normalize following prolactin normalization; confirms cabergoline as first-line pharmacological prolactin control; early gyno intervention with SERMs (tamoxifen/raloxifene) reverses small lumps; established gyno requires surgical correction https://pmc.ncbi.nlm.nih.gov/articles/PMC12227483/
SECTION 4 — Side Effect 4: Cholesterol Degradation
[7] Kanayama G et al. — PMC / Frontiers in Neuroendocrinology, 2022 Anabolic–androgenic steroids: How do they work and what are the risks? — AAS increase hepatic lipase (HL) activity; HL converts large HDL2 particles to smaller, rapidly cleared HDL3; LDL increases via stimulation of IDL-to-LDL conversion and inhibition of hepatic LDL receptor; HDL reductions of 39–70% and LDL increases of 11–100% documented; mechanism confirmed via hepatic lipase activity studies; androgenic potency correlates with lipid disruption severity https://pmc.ncbi.nlm.nih.gov/articles/PMC9837614/
[8] Vance DE et al. — Metabolism / PubMed, 1987 The dyslipoproteinemia of anabolic steroid therapy: increase in hepatic triglyceride lipase precedes the decrease in high density lipoprotein2 cholesterol — stanozolol administration increased HTGL activity 62% on day 1, 230% by day 3; HDL dropped 39% by day 7; confirms hepatic lipase induction as primary mechanism of AAS-induced HDL reduction; temporal relationship established (HTGL rises before HDL falls); reversibility confirmed after discontinuation https://pubmed.ncbi.nlm.nih.gov/3657514/
SECTION 5 — Side Effect 5: Elevated Blood Pressure
[9] Liu JD & Wu YQ — Chinese Medical Journal / PMC, 2019 Anabolic-androgenic steroids and cardiovascular risk — AAS increase blood pressure via multiple mechanisms: erythrocytosis (increased RBC production thickening blood), sodium retention via renal effects, and arterial stiffness from cholesterol-driven vascular changes; hypertension significantly increases cardiovascular event risk; AAS-induced hypertension documented alongside cardiac hypertrophy and atherosclerosis; ARBs and ACE inhibitors recommended for pharmacological management https://pmc.ncbi.nlm.nih.gov/articles/PMC6797160/
SECTION 6 — Side Effect 6: Psychological Disorders
[10] Carbone EA et al. — MDPI Brain Sciences, 2025 Anabolic–Androgenic Steroids and Brain Damage: A Review of Evidence and Medico-Legal Implications — chronic AAS exposure disrupts serotonin and dopamine systems; structural and functional changes in prefrontal cortex and limbic regions confirmed; increased risk of depression, anxiety, aggression, and psychosis; dopaminergic D2 receptor overstimulation drives aggression observed in AAS abusers; serotonin depletion in amygdala and hypothalamus mediates “tren rage”; psychological symptoms resolve as androgen clears but recovery of neurotransmitter systems takes considerably longer than use period https://www.mdpi.com/2673-6756/5/3/31
[11] Daher JC et al. — PMC / Molecular Neurobiology, 2018 The Role of Anabolic Androgenic Steroids in Disruption of the Physiological Function in Discrete Areas of the Central Nervous System — AAS alter serotonergic, dopaminergic, and glutamatergic signaling in hypothalamus, amygdala, hippocampus, and prefrontal cortex; anxiety and aggression result from multi-neurotransmitter disruption; spectrum from mild irritability to psychosis and suicidal ideation documented; unpredictable individual response; dose-dependent severity https://pmc.ncbi.nlm.nih.gov/articles/PMC5994209/
SECTION 7 — Side Effect 7: Testosterone Suppression
[12] Kanayama G et al. — PMC / Psychiatry and Clinical Neurosciences, 2015 Prolonged Hypogonadism in Males Following Withdrawal from Anabolic-Androgenic Steroids — exogenous AAS suppress HPT axis via negative feedback; near-complete shutdown rapid; testosterone levels often <50 ng/dL during use; post-cessation hypogonadism documented for months to years; in one series, AAS-induced hypogonadism accounted for 43% of cases of profound hypogonadism (<50 ng/dL); some cases of permanent Leydig cell damage requiring lifelong TRT https://pmc.ncbi.nlm.nih.gov/articles/PMC4398624/
[13] de Ronde W & Smit DL — PMC / Endocrine Connections, 2023 Physical, psychological and biochemical recovery from anabolic steroid-induced hypogonadism: a scoping review — HPT axis recovery ranges from spontaneous recovery to permanent non-recovery; near-complete testosterone recovery over months; complete gonadotropin recovery expected 3–6 months post-cessation; SERMs (clomiphene, tamoxifen) stimulate LH/FSH to restart testicular production; dose, duration, and age at cessation determine recovery timeline and success https://pmc.ncbi.nlm.nih.gov/articles/PMC10620455/
SECTION 8 — Side Effect 8: Insomnia
[14] Smit DL et al. — PMC / Frontiers in Reproductive Health (HAARLEM Study), 2021 Anabolic Androgenic Steroids Induce Reversible Left Ventricular Hypertrophy and Cardiac Dysfunction — prospective study; AAS cycle of median 16 weeks produced significant CNS stimulation documented alongside cardiac changes; insomnia and night sweats among commonly reported side effects; thermoregulation disruption confirmed; symptoms resolved after cessation and recovery period; reversibility confirmed at 1-year follow-up https://pmc.ncbi.nlm.nih.gov/articles/PMC9580689/
[15] Birgner C et al. — Brain Research / PubMed reference via PMC review Anabolic androgenic steroids cause long-standing changes in the brain — serotonin system recovery lasts approximately 6x the duration of administration period; dopamine system recovery takes ~5x the administration period; CNS maintained in alert state during use (explaining insomnia mechanism); neurotransmitter disruption persists substantially longer than the active substance; sleep normalization follows hormone clearance https://dopinglinkki.fi/en/info-bank/other-information/anabolic-steroids-cause-long-standing-changes-in-the-brain/
SECTION 9 — Side Effect 9: Cardiovascular System Damage
[16] Baggish AL et al. — Circulation, 2017 Cardiovascular toxicity of illicit anabolic-androgenic steroid use — 86 long-term AAS users (mean 7 years) vs. 54 non-users assessed by coronary CT angiography; AAS users had higher coronary plaque volume and earlier MI rates; dose-dependent relationship between cumulative AAS duration and atherosclerosis severity confirmed; structural cardiac abnormalities including LV hypertrophy, ventricular dysfunction, and arterial stiffness documented; some changes persist after cessation https://pubmed.ncbi.nlm.nih.gov/28461338/
[17] Pergolini I et al. — MDPI Biomedicines, 2025 Anabolic–Androgenic Steroids Induced Cardiomyopathy: A Narrative Review — comprehensive review of AAS cardiovascular mechanisms: oxidative stress, androgen receptor overactivation on cardiomyocytes, RAAS dysregulation, pro-apoptotic signaling; LV hypertrophy, myocardial fibrosis, atherosclerosis, arterial stiffness, and prothrombotic state documented; endothelial dysfunction via nitric oxide inhibition confirmed; HDL reduction and LDL increase compound atherogenic risk; some structural damage irreversible after prolonged use https://www.mdpi.com/2227-9059/13/9/2190
[18] Smit DL et al. — Circulation AHA / Danish Registry Study, 2024 Cardiovascular Disease in Anabolic Androgenic Steroid Users — large Danish population-based cohort; AAS users sanctioned in antidoping program followed until 2023; significantly elevated incidence of cardiovascular disease vs. age/sex-matched controls; atrial fibrillation, LV hypertrophy, and sudden cardiac death documented; erythrocytosis-driven thromboembolism risk confirmed; increased long-term cardiovascular mortality even years after cessation https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.124.071117




Leave a Reply
You must be logged in to post a comment.