
Exhausted all the time? Can’t handle stress anymore? Your doctor says your tests are normal but you feel terrible.
You’re constantly tired. You need coffee just to function. Small stressors feel overwhelming.
You Google your symptoms. “Adrenal fatigue” pops up everywhere. It sounds exactly like what you’re experiencing.
You see the symptoms listed:
- Extreme fatigue not improved by sleep
- Difficulty waking up in the morning
- Craving salt and sugar
- Low blood pressure
- Brain fog and poor concentration
- Weakened immune system
That’s you. Every single symptom. But your doctor dismisses it completely.
Here’s what’s actually happening: “Adrenal fatigue” isn’t a recognized medical diagnosis because your adrenal glands don’t actually “fatigue” or “burn out” from stress. However, chronic stress DOES dysregulate your HPA axis (hypothalamic-pituitary-adrenal axis), creating real symptoms that desperately need addressing. The fatigue is real. The mechanism is just misunderstood. And fixing it requires understanding what’s truly broken.
In this comprehensive guide, I’ll explain why “adrenal fatigue” isn’t scientifically accurate (but why you still feel terrible), reveal what chronic stress actually does to your endocrine system (HPA axis dysregulation), show you the 7 real conditions that cause “adrenal fatigue” symptoms (most doctors miss these), provide the complete diagnostic protocol to find what’s actually wrong (proper testing), and give you the evidence-based treatment plan that actually works (not expensive supplements).
Whether you’re exhausted, overwhelmed, or just want to understand your stress response system, this article reveals the truth.
Let’s fix what’s really broken in your stress system.
TABLE OF CONTENTS
What Is “Adrenal Fatigue” and Why Is It Controversial?
Understanding the debate.
The “Adrenal Fatigue” Theory
The claim:
- Prolonged stress “exhausts” your adrenal glands
- Adrenals can’t produce enough cortisol
- This causes chronic fatigue and other symptoms
- Common in modern high-stress lifestyle
- Sounds logical
Who promotes it:
- Alternative medicine practitioners
- Functional medicine doctors
- Naturopaths
- Supplement companies
- Non-mainstream medicine
The proposed symptoms:
- Constant fatigue (not improved by sleep)
- Difficulty waking in morning (need multiple alarms)
- Afternoon energy crash (3-4 PM collapse)
- Evening energy surge (second wind at night)
- Salt cravings (can’t stop eating salty foods)
- Sugar cravings (need constant snacks)
- Low blood pressure (dizzy when standing)
- Poor stress tolerance (everything feels overwhelming)
- Brain fog (can’t think clearly)
- Weakened immunity (catch every cold)
- Long list of vague symptoms
The proposed treatment:
- Expensive supplements (adrenal “support”)
- Specific diet protocols
- Stress reduction
- Lifestyle changes
- Costly interventions
Why Mainstream Medicine Rejects It
The scientific consensus:
- No evidence adrenal glands “fatigue”
- Adrenal insufficiency (real disease) is different
- Cortisol levels typically normal in these patients
- Blood tests don’t support diagnosis
- Not recognized by Endocrine Society
The organizations that reject it:
- Endocrine Society (hormone specialists)
- American Association of Clinical Endocrinologists
- Most conventional medicine doctors
- Medical establishment unanimous
Why doctors are skeptical:
- Vague, non-specific symptoms
- No objective diagnostic criteria
- Normal lab tests in most cases
- Term used to sell expensive supplements
- Lacks scientific rigor
The studies:
- Multiple systematic reviews
- No evidence for “adrenal fatigue” as distinct condition
- Cortisol levels normal or even elevated in stressed individuals
- Science doesn’t support theory
The Problem With Both Sides
Alternative medicine’s mistake:
- Wrong mechanism (adrenals don’t “fatigue”)
- Oversimplified explanation
- Expensive unnecessary supplements
- Right symptoms, wrong explanation
Conventional medicine’s mistake:
- Dismissing real symptoms
- “Your labs are normal, nothing’s wrong”
- Not investigating underlying causes
- Leaving patients suffering
- Right science, poor patient care
The truth in the middle:
- Symptoms are REAL
- Suffering is REAL
- But mechanism is misunderstood
- Need accurate diagnosis
- Both sides partially right
What’s Actually Happening: HPA Axis Dysregulation
The real mechanism behind your symptoms.
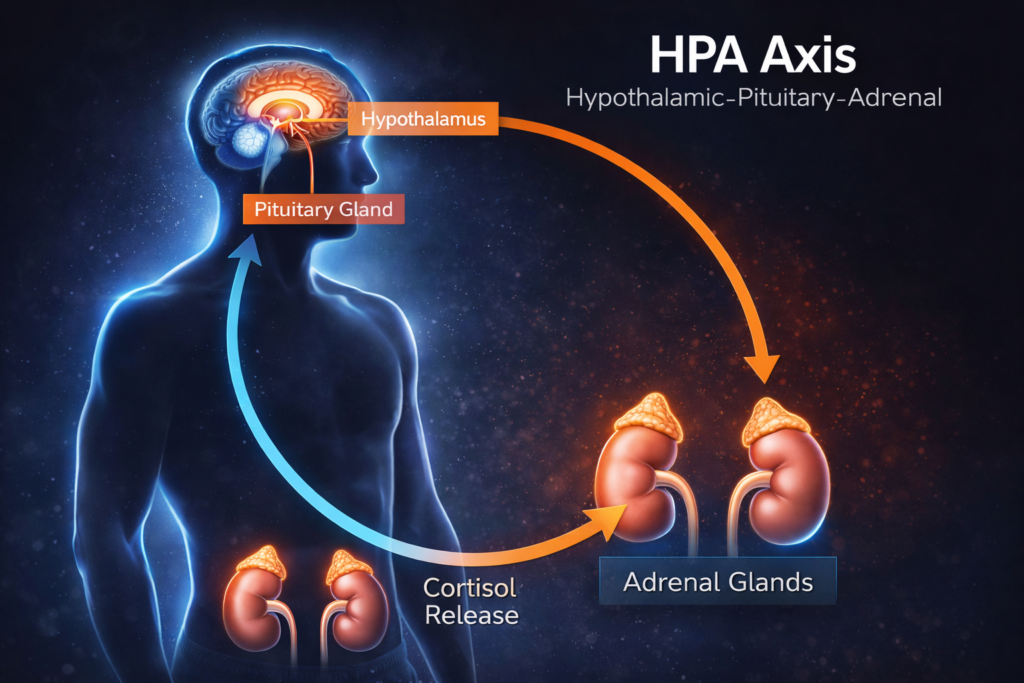
Understanding the HPA Axis
What it is:
- Hypothalamic-Pituitary-Adrenal axis
- Your body’s stress response system
- Complex feedback loop
- Central stress control
The components:
Hypothalamus (brain):
- Detects stress
- Releases CRH (corticotropin-releasing hormone)
- Stress detector
Pituitary gland (brain):
- Receives CRH signal
- Releases ACTH (adrenocorticotropic hormone)
- Stress messenger
Adrenal glands (above kidneys):
- Receive ACTH signal
- Produce cortisol (stress hormone)
- Stress responders
The feedback loop:
- Cortisol signals back to brain
- “We have enough cortisol, stop producing”
- Negative feedback
- Self-regulating system
- Like a thermostat
How Chronic Stress Breaks the System
Acute stress (normal):
- Stressor appears (deadline, threat, exercise)
- HPA axis activates
- Cortisol rises appropriately
- Stressor resolves
- Cortisol returns to baseline
- System resets
- Healthy response
Chronic stress (problematic):
- Constant stressors (work, relationships, financial)
- HPA axis constantly activated
- Cortisol chronically elevated or dysregulated
- Feedback loop becomes impaired
- System can’t reset properly
- Dysregulated response
What happens over time:
Phase 1: Alarm (hyperarousal):
- Initial stress response
- Cortisol elevated
- Feel “wired and tired”
- Sleep disruption
- System on high alert
Phase 2: Resistance (adaptation):
- Body tries to adapt
- Cortisol patterns flatten
- Morning cortisol lower
- Evening cortisol higher
- Rhythm disrupted
Phase 3: Exhaustion (dysregulation):
- Not “fatigue” but dysregulation
- Cortisol levels may be normal or low-normal
- But rhythm completely disrupted
- Poor stress response
- System confused
The key point:
- Adrenals still PRODUCE cortisol
- Not “fatigued” or “burned out”
- But RHYTHM is disrupted
- Response is dysregulated
- Wrong pattern, not low output
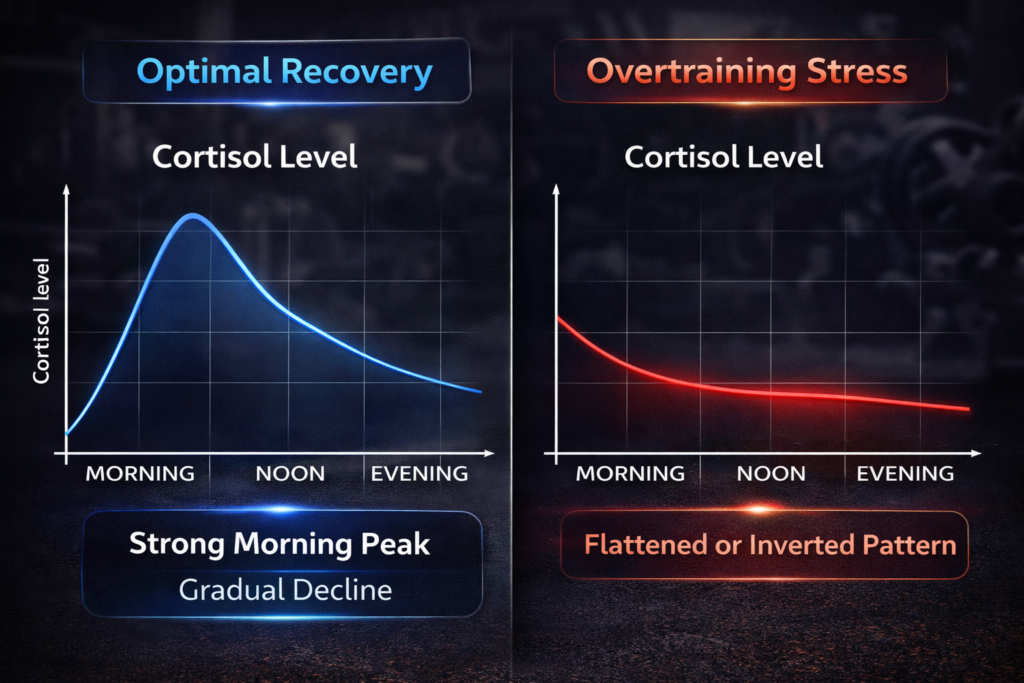
The Real Problems
Problem 1: Cortisol rhythm disruption
- Normal: High morning, low evening
- Dysregulated: Flat all day, or reversed
- This causes symptoms
- Timing is everything
Problem 2: Poor cortisol response
- Should rise appropriately to stress
- Dysregulated: Blunted response or overreaction
- Can’t handle stress normally
- Response impaired
Problem 3: Impaired negative feedback
- Brain doesn’t “hear” cortisol signal properly
- Keeps producing even when shouldn’t
- Or doesn’t produce when should
- Communication breakdown
Problem 4: Downstream effects
- Thyroid function affected
- Sex hormone production affected
- Immune function affected
- Sleep disrupted
- Cascade of problems
Why “adrenal fatigue” stuck:
- Describes how people FEEL
- Exhaustion is accurate description
- Easy to understand
- But mechanism is wrong
- Good description, bad science
The better term:
- HPA axis dysregulation
- Hypothalamic-pituitary-adrenal dysfunction
- Maladaptive stress response
- More accurate
The 7 Real Conditions Causing Your Symptoms
What might actually be wrong.

Condition 1: Subclinical Hypothyroidism
What it is:
- Thyroid producing slightly low hormone
- Not low enough for “official” diagnosis
- But enough to cause symptoms
- Gray area thyroid dysfunction
Why it mimics “adrenal fatigue”:
- Extreme fatigue
- Weight gain
- Cold intolerance
- Brain fog
- Depression
- Nearly identical symptoms
The testing problem:
- Standard test: TSH only
- TSH can be “normal” while free T3/T4 low
- Doctors say “you’re fine”
- But you’re not
- Incomplete testing
What to test:
- TSH (should be 0.5-2.5, not just <4.5)
- Free T3
- Free T4
- Thyroid antibodies (TPO, TG)
- Reverse T3
- Complete thyroid panel
Risk factors:
- Family history
- Autoimmune conditions
- Chronic stress (suppresses thyroid)
- Iodine deficiency
- Common in stressed individuals
Condition 2: Iron Deficiency (Without Anemia)
What it is:
- Low iron stores (ferritin)
- But hemoglobin still normal
- Not “anemia” by standard definition
- Pre-anemic iron deficiency
Why it mimics “adrenal fatigue”:
- Extreme fatigue
- Exercise intolerance
- Brain fog
- Cold intolerance
- Looks exactly like adrenal fatigue
The testing problem:
- Standard test: Hemoglobin/hematocrit only
- These can be normal with low ferritin
- Ferritin not routinely checked
- Missed diagnosis
What to test:
- Ferritin (should be 50-100+ ng/mL, not just >12)
- Iron
- TIBC
- Transferrin saturation
- Complete iron panel
Who’s at risk:
- Menstruating women (monthly blood loss)
- Athletes (increased iron needs)
- Vegetarians/vegans (less absorbable iron)
- Chronic inflammation (hides iron deficiency)
- Very common
Condition 3: Vitamin D Deficiency
What it is:
- Insufficient vitamin D levels
- Most people deficient (especially winter)
- Affects energy and mood
- Epidemic deficiency
Why it mimics “adrenal fatigue”:
- Fatigue and weakness
- Muscle pain
- Depression
- Immune dysfunction
- Similar symptom profile
The testing problem:
- Not routinely checked
- Standard “normal” range too low (>20 ng/mL)
- Optimal levels higher (40-60 ng/mL)
- Widespread deficiency missed
What to test:
- 25-hydroxyvitamin D
- Should be 40-60 ng/mL
- Simple blood test
Risk factors:
- Limited sun exposure
- Dark skin (in northern climates)
- Indoor lifestyle
- Sunscreen use (blocks production)
- Most people deficient
Condition 4: Sleep Apnea
What it is:
- Breathing repeatedly stops during sleep
- Brief awakenings (often not remembered)
- Disrupts sleep quality severely
- Unrefreshing sleep
Why it mimics “adrenal fatigue”:
- Extreme morning fatigue
- Afternoon energy crashes
- Brain fog
- Difficulty concentrating
- High blood pressure
- Identical symptoms
The testing problem:
- Not considered unless overweight
- Can occur in normal-weight individuals
- Requires specific sleep study
- Often missed
What to test:
- Home sleep study or in-lab polysomnography
- AHI (Apnea-Hypopnea Index)
- Oxygen saturation monitoring
- Specialized testing
Risk factors:
- Overweight/obesity
- Large neck circumference
- Snoring
- Witnessed apneas
- Morning headaches
- Common but undiagnosed
Condition 5: Depression and Anxiety
What it is:
- Clinical depression or anxiety disorders
- Can manifest physically
- Often stress-related
- Mental health manifesting physically
Why it mimics “adrenal fatigue”:
- Fatigue and low energy
- Difficulty concentrating
- Sleep problems
- Appetite changes
- Physical symptoms
- Overlapping presentation
The testing problem:
- No blood test for depression
- Symptoms dismissed as “stress”
- Stigma prevents seeking help
- Clinical diagnosis missed
What to assess:
- PHQ-9 (depression screening)
- GAD-7 (anxiety screening)
- Clinical interview
- Mental health evaluation
Important note:
- Not “all in your head”
- Real neurotransmitter dysfunction
- Treatable condition
- Affects physical health
- Biological disease
Condition 6: Chronic Inflammation
What it is:
- Persistent low-grade inflammation
- From various sources
- Affects energy and wellbeing
- Silent inflammatory state
Why it mimics “adrenal fatigue”:
- Fatigue
- Malaise
- Brain fog
- Sleep disruption
- Immune dysfunction
- Inflammatory symptoms
Common causes:
- Poor diet (processed foods, sugar)
- Gut dysbiosis
- Food sensitivities
- Chronic infections
- Autoimmune conditions
- Multiple sources
What to test:
- High-sensitivity CRP
- ESR
- Ferritin (also inflammation marker)
- Homocysteine
- Inflammatory markers
Treatment focus:
- Address underlying cause
- Anti-inflammatory diet
- Gut healing
- Stress management
- Root cause approach
Condition 7: Blood Sugar Dysregulation
What it is:
- Reactive hypoglycemia
- Insulin resistance
- Pre-diabetes
- Metabolic dysfunction
Why it mimics “adrenal fatigue”:
- Energy crashes (especially afternoon)
- Sugar cravings
- Shakiness if meals delayed
- Brain fog
- Irritability
- Blood sugar symptoms
The testing problem:
- Fasting glucose can be normal
- HbA1c can be normal
- Need glucose tolerance test or CGM
- Standard tests miss it
What to test:
- Fasting glucose
- Fasting insulin
- HbA1c
- HOMA-IR (calculated)
- Glucose tolerance test
- Comprehensive metabolic testing
The connection:
- Chronic stress increases cortisol
- Cortisol increases blood sugar
- Chronic elevation causes insulin resistance
- Creates energy rollercoaster
- Stress-metabolic connection
Proper Diagnostic Protocol
How to find what’s actually wrong.
Step 1: Comprehensive Blood Work
Essential tests:
Thyroid panel (complete):
- TSH (optimal 0.5-2.5 mIU/L)
- Free T3 (optimal 3.0-4.0 pg/mL)
- Free T4 (optimal 1.0-1.5 ng/dL)
- Reverse T3
- TPO antibodies
- Thyroglobulin antibodies
- Not just TSH
Iron panel (complete):
- Ferritin (optimal 50-100+ ng/mL)
- Serum iron
- TIBC
- Transferrin saturation
- Complete picture
Metabolic panel:
- Fasting glucose
- Fasting insulin
- HbA1c
- HOMA-IR calculation
- Blood sugar assessment
Inflammatory markers:
- High-sensitivity CRP
- ESR
- Homocysteine
- Inflammation check
Vitamins and minerals:
- Vitamin D (25-OH)
- Vitamin B12
- Folate
- Magnesium (RBC, not serum)
- Zinc
- Nutrient status
Hormones (if indicated):
- Cortisol (morning and evening)
- DHEA-S
- Sex hormones (if relevant symptoms)
- Endocrine assessment
CBC (complete blood count):
- Hemoglobin
- Hematocrit
- WBC
- Platelets
- General health markers
The problem:
- Most doctors order minimal labs
- “Comprehensive metabolic panel” isn’t comprehensive
- Need to specifically request these tests
- Advocate for yourself
Step 2: Cortisol Assessment (If Needed)
When to test cortisol:
- After ruling out other conditions
- If symptoms persist
- If truly suspect HPA dysregulation
- Not first-line testing
The right way to test:
Four-point salivary cortisol:
- Upon waking (should be high)
- Noon (moderate)
- Afternoon (lower)
- Before bed (low)
- Shows daily rhythm
- Pattern matters more than absolute levels
Why NOT just one morning blood test:
- Single blood test shows one moment
- Doesn’t show rhythm
- Venipuncture is stressor (falsely elevates)
- Misses pattern
- Incomplete picture
What to look for:
- Flattened curve (all same level)
- Reversed pattern (low morning, high evening)
- Exaggerated response
- Pattern abnormalities
Important caveat:
- Even if pattern abnormal
- Doesn’t mean adrenals “fatigued”
- Means HPA axis dysregulated
- Need to find WHY
- Symptom of underlying problem
Step 3: Sleep Assessment
If fatigue primary symptom:
- Sleep study essential
- Home sleep test or in-lab
- Check for apnea, restless legs, etc.
- Rule out sleep disorders
Sleep diary:
- Track sleep patterns 2 weeks
- Bedtime, wake time
- Sleep quality
- Energy levels
- Identify patterns
Sleep hygiene assessment:
- Bedroom environment
- Pre-bed routine
- Screen time
- Caffeine timing
- Lifestyle factors
Step 4: Mental Health Screening
Depression screening:
- PHQ-9 questionnaire
- Clinical interview
- Assess for major depression
- Don’t overlook mental health
Anxiety screening:
- GAD-7 questionnaire
- Assess for anxiety disorders
- PTSD screening if trauma history
- Comprehensive assessment
The importance:
- Depression and anxiety are PHYSICAL
- Affect energy, sleep, appetite
- Treatable conditions
- Not “just stress”
- Real medical conditions
Step 5: Lifestyle Assessment
Stress inventory:
- Work stress
- Relationship stress
- Financial stress
- Health stress
- Identify stressors
Diet assessment:
- Food diary 3-7 days
- Eating patterns
- Nutrient quality
- Blood sugar patterns
- Nutrition evaluation
Exercise assessment:
- Type, frequency, intensity
- Overtraining or undertraining
- Recovery adequacy
- Activity level
Sleep assessment:
- Hours per night
- Quality
- Consistency
- Sleep quantity and quality
The Evidence-Based Treatment Plan
What actually works to fix the real problems.

Foundation: Address Underlying Conditions
If hypothyroidism:
- Thyroid hormone replacement (if needed)
- Selenium supplementation (200mcg daily)
- Iodine adequate but not excessive
- Reduce goitrogens if Hashimoto’s
- Thyroid optimization
If iron deficiency:
- Iron supplementation (65-130mg elemental iron daily)
- Vitamin C with iron (enhances absorption)
- Take away from coffee/tea
- Monitor ferritin every 3 months
- Replenish stores
If vitamin D deficiency:
- Vitamin D3 supplementation (2000-5000 IU daily)
- With K2 (for proper calcium regulation)
- Recheck levels in 3 months
- Optimize levels
If sleep apnea:
- CPAP machine (if severe)
- Oral appliance (if mild-moderate)
- Weight loss (if overweight)
- Positional therapy
- Treat sleep disorder
If depression/anxiety:
- Therapy (CBT highly effective)
- Medication if indicated
- Regular exercise
- Stress management
- Mental health treatment
If chronic inflammation:
- Anti-inflammatory diet
- Address gut health
- Remove inflammatory triggers
- Omega-3 supplementation
- Reduce inflammation
If blood sugar dysregulation:
- Low-glycemic diet
- Protein at every meal
- Regular meals (no skipping)
- Exercise (improves insulin sensitivity)
- Stabilize blood sugar
Universal Strategies (Everyone Benefits)
Strategy 1: Optimize Sleep
Why it’s critical:
- Sleep deprivation disrupts ALL hormones
- Cortisol, thyroid, growth hormone affected
- Can’t heal without proper sleep
- Foundation of recovery
The protocol:
- 7-9 hours nightly (non-negotiable)
- Consistent schedule (same bedtime/wake time)
- Dark room (blackout curtains)
- Cool temperature (65-68°F)
- No screens 1 hour before bed
- No caffeine after 2 PM
- Sleep hygiene essentials
If struggling:
- Magnesium glycinate (400mg before bed)
- Melatonin (0.5-3mg, start low)
- L-theanine (200mg)
- Sleep study if not improving
- Supplement support
Strategy 2: Manage Stress Effectively
Why it’s critical:
- Chronic stress is root cause
- Can’t heal while stressed
- Must address directly
- Cannot be skipped
Daily practices:
Meditation (proven effective):
- 10-20 minutes daily
- Reduces cortisol significantly
- Improves HPA axis function
- Apps: Headspace, Calm, Insight Timer
- Evidence-based stress reduction
Deep breathing:
- Box breathing (4-4-4-4)
- 4-7-8 breathing
- 5-10 minutes, 2-3x daily
- Activates parasympathetic nervous system
- Immediate stress relief
Nature exposure:
- 20-30 minutes outdoors daily
- Walking in nature ideal
- Reduces cortisol
- Improves mood
- Natural stress reducer
Social connection:
- Regular meaningful interaction
- Strong predictor of health
- Reduces stress response
- Social support matters
What NOT to do:
- Excessive exercise (adds stress)
- Overcommitment (more stress)
- Stimulants to push through
- Ignoring the problem
- Avoid making it worse
Strategy 3: Optimize Nutrition
Why it matters:
- Blood sugar stability critical
- Nutrient deficiencies worsen symptoms
- Inflammation from poor diet
- Food is medicine
The approach:
Blood sugar stability:
- Protein at every meal (30-40g)
- Pair carbs with protein/fat
- Regular meal timing
- Avoid long fasting
- Stable energy
Anti-inflammatory diet:
- Whole foods focus
- Omega-3 rich (fatty fish 2-3x weekly)
- Colorful vegetables (antioxidants)
- Limit processed foods
- Reduce sugar
- Reduce inflammation
Adequate calories:
- Don’t undereat (adds stress)
- Match energy expenditure
- Don’t create additional stress
- Sufficient fuel
Hydration:
- Half body weight in ounces minimum
- More if exercising or hot climate
- Proper hydration supports all function
- Basic but critical
Strategy 4: Exercise Appropriately
Why it matters:
- Moderate exercise helps
- Excessive exercise worsens problem
- Need to find balance
- Goldilocks zone
What works:
Resistance training:
- 3-4x per week
- 45-60 minutes
- Progressive overload
- Adequate recovery
- Builds resilience
Walking:
- 30-60 minutes daily
- Low stress activity
- Sunshine and nature bonus
- Sustainable activity
Yoga:
- Gentle to moderate intensity
- Stress reduction
- Improves flexibility
- Mind-body connection
What doesn’t work:
- Hours of cardio daily
- Training through exhaustion
- No rest days
- Overtraining
- Makes problem worse
The key:
- Exercise should energize, not exhaust
- If exhausted after, doing too much
- Recovery is when adaptation happens
- Quality over quantity
Supplement Protocol (Evidence-Based Only)
Tier 1: Strong evidence
Magnesium glycinate:
- 400mg before bed
- Most people deficient
- Supports sleep and stress response
- Calming effect
- Nearly universal benefit
Omega-3 fish oil:
- 2-3g EPA+DHA daily
- Reduces inflammation
- Supports brain health
- Well-researched
Vitamin D3 (if deficient):
- 2000-5000 IU daily
- With vitamin K2
- Monitor levels
- If tested low
Adaptogenic herbs (moderate evidence):
Rhodiola rosea:
- 200-400mg daily
- Improves stress resilience
- Reduces fatigue
- Some research support
- May help
Ashwagandha:
- 300-600mg daily
- Reduces cortisol
- Improves stress response
- Several studies
- Promising
What NOT to waste money on:
- “Adrenal support” complexes (no evidence)
- Adrenal glandulars (no evidence)
- Licorice root (dangerous long-term)
- Most marketed “adrenal supplements”
- Save your money
Timeline for Recovery
What to expect:
Week 1-2:
- Minimal improvement
- Implementing changes
- Building foundation
- Patience required
Week 3-4:
- Slight energy improvement
- Sleep beginning to improve
- Less overwhelm
- Early signs
Month 2-3:
- Noticeable energy increase
- Better stress tolerance
- Improved mood
- Meaningful progress
Month 4-6:
- Significant improvement
- Energy normalized
- Stress response healthy
- Major recovery
Month 6-12:
- Full recovery possible
- Maintained with lifestyle
- New baseline established
- Long-term success
The reality:
- Takes time to heal
- Didn’t develop overnight
- Won’t resolve overnight
- Consistency is key
- Patience and persistence
Why Supplements Marketed for “Adrenal Fatigue” Don’t Work
The truth about expensive supplements.
The Marketing
What they claim:
- “Support” adrenal glands
- “Nourish” adrenals
- “Restore” adrenal function
- Contain “adrenal extract” or glandulars
- Vague promises
Common ingredients:
- Adrenal glandulars (bovine adrenal tissue)
- Vitamin C (high dose)
- B vitamins (high dose)
- Licorice root
- Various adaptogens
- Expensive formulas
The cost:
- $30-80 per month
- Multiple bottles often recommended
- “Take for 6-12 months”
- Significant financial burden
Why They Don’t Work
Reason 1: Adrenals don’t need “support”
- They’re not fatigued
- They’re dysregulated
- Giving them “nutrients” doesn’t fix regulation
- Wrong target
Reason 2: Glandulars are nonsense
- Bovine adrenal tissue
- Digested in stomach
- Doesn’t reach your adrenals
- No evidence of benefit
- Biologically implausible
Reason 3: High-dose vitamins unnecessary
- If not deficient, excess doesn’t help
- May even cause harm
- Test first, supplement deficiencies
- Shotgun approach doesn’t work
Reason 4: Licorice root is dangerous
- Can raise blood pressure
- Causes potassium loss
- Mimics aldosterone
- Not fixing root cause
- Potential harm
Reason 5: Expensive adaptogens
- Modest effects at best
- Not addressing underlying cause
- Rhodiola and ashwagandha may help
- But don’t need expensive formulas
- Overpriced
The Better Approach
Spend money on:
- Proper lab testing (find real problem)
- Quality sleep environment
- Whole food groceries
- Stress management resources (therapy, classes)
- Address root causes
Don’t spend money on:
- “Adrenal support” supplements
- Glandular products
- Expensive proprietary formulas
- Monthly subscriptions
- Unproven interventions
When to See a Doctor (And What Kind)
Getting proper medical care.
Warning Signs (Seek Care Immediately)
Severe symptoms:
- Extreme weakness (can’t perform daily activities)
- Significant unintentional weight loss
- Very low blood pressure (dizzy when standing)
- Darkening of skin (hyperpigmentation)
- Salt craving so intense it’s abnormal
- Nausea and vomiting
- Could be Addison’s disease
Addison’s disease:
- Real adrenal insufficiency
- Life-threatening condition
- Adrenals truly don’t produce cortisol
- Requires immediate medical attention
- Medical emergency
The difference:
- “Adrenal fatigue” → Normal cortisol, dysregulated pattern
- Addison’s disease → Actually LOW cortisol, dangerous
- One is myth, one is emergency
Finding the Right Doctor
Start with:
Primary care physician:
- Initial workup
- Basic lab testing
- Rule out common causes
- Refer if needed
- First stop
If initial workup normal but symptoms persist:
Endocrinologist:
- Hormone specialist
- Comprehensive endocrine testing
- Diagnose thyroid, diabetes, etc.
- Hormone expert
Integrative/Functional medicine doctor:
- Looks at complete picture
- More comprehensive testing
- Addresses root causes
- Combines conventional and holistic
- Whole-person approach
Sleep medicine specialist:
- If fatigue primary symptom
- Sleep study
- Diagnose sleep disorders
- Sleep expert
Psychiatrist/Psychologist:
- If depression/anxiety suspected
- Comprehensive mental health evaluation
- Evidence-based treatment
- Mental health expert
What to Ask Your Doctor
For testing:
- “Can we do comprehensive thyroid panel, not just TSH?”
- “Can we check ferritin and complete iron panel?”
- “Can we test vitamin D and B12?”
- “Can we check fasting glucose AND insulin?”
- Advocate for thorough testing
For referrals:
- “If these tests are normal, can you refer me to [specialist]?”
- “Can I get a sleep study?”
- “Should I see an endocrinologist?”
- Don’t accept dismissal
What NOT to say:
- “I think I have adrenal fatigue”
- This immediately discredits you
- Doctor will dismiss
- Use proper terminology
What TO say:
- “I’m experiencing severe fatigue and symptoms of possible HPA axis dysregulation”
- “I want to rule out thyroid, iron deficiency, sleep disorders”
- “Can we do comprehensive testing?”
- Professional language
The Bottom Line: It’s Real, But Misunderstood
After explaining everything:
The truth about “adrenal fatigue”:
✅ Your symptoms are REAL (not imagined or psychological)
✅ “Adrenal fatigue” is NOT scientifically accurate (adrenals don’t fatigue)
✅ HPA axis dysregulation is real (stress system dysfunction)
✅ Multiple conditions cause identical symptoms (need proper diagnosis)
✅ Treatment addresses root causes, not adrenals (systemic approach)
Key takeaways:
What “adrenal fatigue” actually is:
- Collection of symptoms
- Caused by various conditions
- HPA axis dysregulation common
- Chronic stress a factor
- But adrenals aren’t “fatigued”
- Misnamed condition
What might really be wrong:
- Subclinical hypothyroidism (thyroid slightly low)
- Iron deficiency without anemia (low ferritin)
- Vitamin D deficiency (very common)
- Sleep apnea (unrefreshing sleep)
- Depression/anxiety (physical manifestation)
- Chronic inflammation (various sources)
- Blood sugar dysregulation (energy crashes)
- Need proper diagnosis
Proper diagnostic approach:
- Comprehensive blood work (thyroid, iron, vitamins, glucose, inflammation)
- Four-point salivary cortisol (if indicated, after ruling out other causes)
- Sleep study (if appropriate)
- Mental health screening (don’t overlook)
- Lifestyle assessment (identify stressors)
- Find real cause
Evidence-based treatment:
- Address underlying condition (thyroid, iron, vitamin D, etc.)
- Optimize sleep (7-9 hours, non-negotiable)
- Manage stress (meditation, breathing, nature)
- Optimize nutrition (blood sugar stability, anti-inflammatory)
- Exercise appropriately (moderate, not excessive)
- Targeted supplements only (magnesium, omega-3, vitamin D if deficient)
- Systemic approach
What doesn’t work:
- “Adrenal support” supplements (no evidence)
- Glandular products (not physiologically sound)
- Expensive proprietary formulas (waste of money)
- Ignoring underlying causes (symptoms persist)
- Save your money
Timeline for recovery:
- Week 1-2: Foundation building
- Week 3-4: Early improvements
- Month 2-3: Noticeable progress
- Month 4-6: Significant recovery
- Month 6-12: Full recovery possible
- Requires patience
When to seek medical care:
- Severe symptoms (weakness, weight loss, very low BP)
- Could be Addison’s disease (real adrenal insufficiency)
- Life-threatening emergency
- See doctor immediately
- Don’t delay if severe
Finding the right doctor:
- Start: Primary care (initial workup)
- If needed: Endocrinologist (hormones), sleep specialist (sleep disorders), integrative doctor (comprehensive), psychiatrist (mental health)
- Advocate for comprehensive testing
- Don’t accept dismissal
- Persist until diagnosed
YOUR SYMPTOMS ARE REAL. THE CAUSE IS MISUNDERSTOOD. PROPER DIAGNOSIS AND TREATMENT WORK.
Ready to build a complete recovery plan with proper medical testing, evidence-based interventions, lifestyle optimization strategies, and sustainable habits that address the root cause of your fatigue instead of expensive supplements that don’t work? Understanding what’s really wrong is just the beginning. Get a comprehensive guide to working with your doctor effectively, implementing proven treatment protocols, optimizing all aspects of health systematically, and achieving full recovery. Stop wasting money on “adrenal support.” Start addressing what’s actually broken.





Leave a Reply
You must be logged in to post a comment.