
Think steroids will keep you young and jacked forever? They’re actually aging you faster at the cellular level. Here’s the science you need to know.
You see someone who’s been using steroids for years. They’re 30 but look 45. Harsh facial features. Balding. Weathered skin.
You think “that won’t happen to me” or “they just had bad genetics.” But you’re wrong about how inevitable this is.
You believe:
- Testosterone is anti-aging (TRT ads say so)
- More hormones = better health
- Only extreme doses cause problems
- Aging effects are just cosmetic
Most of this is dangerously wrong. The truth: Using hormones at replacement levels (TRT) can be rejuvenating. Using supraphysiological doses (steroid abuse) accelerates aging at multiple levels: oxidative stress damages cells, organ overload wears out vital systems, cardiovascular damage ages arteries 20-30 years prematurely, telomere shortening speeds cellular aging, and brain atrophy causes cognitive decline. The damage is dose-dependent (more = worse), cumulative (builds over time), and partially irreversible. This isn’t scare tactics. This is documented science.
In this comprehensive guide, I’ll explain the cellular mechanisms of steroid-induced aging (oxidative stress, telomere damage, organ stress), reveal the visible signs (facial changes, hair loss, cardiovascular aging), show you the brain impact (cognitive decline and atrophy), provide harm reduction strategies (if you insist on using), address TRT vs. abuse (the critical dose difference), and answer common questions (reversibility, genetics, safer protocols).
Whether you’re considering steroids, currently using, or trying to understand the long-term consequences, this information is critical.
Let’s examine how steroids age you from the inside out.
TABLE OF CONTENTS
The Paradox: Anti-Aging vs. Accelerated Aging
Understanding the contradiction.
Why Testosterone Is Marketed as Anti-Aging
The TRT claims:
- Increases muscle mass (fights sarcopenia)
- Improves bone density (prevents osteoporosis)
- Enhances energy and mood
- Supports cognitive function
- Improves metabolic health
- Legitimate benefits at replacement doses
The research on TRT (actual replacement):
- Men with clinically low testosterone benefit from replacement
- Brings levels to normal physiological range (300-1000 ng/dL)
- Can improve markers of aging when deficient
- Evidence-based medicine
The key distinction:
- TRT: Replacing what’s missing (therapeutic)
- Steroid abuse: Adding far beyond normal (supraphysiological)
- Completely different scenarios
The Critical Quote
PhD Gabriel Kaminski’s explanation:
- “Using hormones in the context of hormone replacement (TRT) rejuvenates.”
- “Using more hormones than you need ages you.”
- Dose makes the poison
The threshold:
- Normal physiological range: Health-promoting
- Supraphysiological doses: Aging-accelerating
- Clear dividing line
The analogy:
- Water: Essential for life
- Too much water: Drowns you
- Hormones work the same way
- Dose-response relationship
How Steroids Accelerate Aging (The Mechanisms)
The cellular and systemic damage.
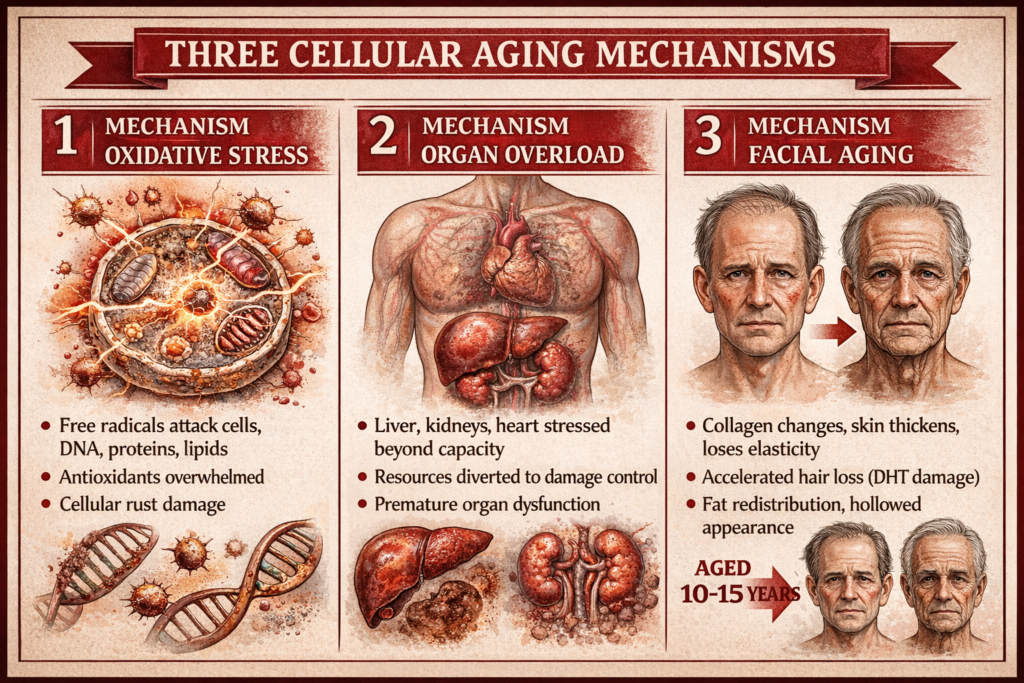
Mechanism 1: Oxidative Stress
What oxidative stress is:
- Imbalance between free radicals (reactive oxygen species) and antioxidants
- Free radicals damage cells, proteins, DNA
- Body can’t neutralize them fast enough
- Cellular rust
The analogy:
- Like metal rusting
- Oxidation damages cellular machinery
- Shortens lifespan of vital components
- Accelerated degradation
How steroids increase oxidative stress:
Increased metabolic activity:
- More muscle mass = higher metabolic rate
- More cellular processes = more free radicals produced
- Body’s antioxidant systems overwhelmed
- Production exceeds clearance
Direct hormonal effects:
- Androgens increase mitochondrial activity
- More energy production = more oxidative byproducts
- Electron transport chain leaks more free radicals
- Mitochondrial stress
The consequences:
- DNA damage (mutation risk, telomere damage)
- Protein dysfunction (enzymes don’t work properly)
- Lipid peroxidation (cell membranes damaged)
- Accelerated cellular aging
- Widespread damage
The research:
- Steroid users show elevated markers of oxidative stress
- Decreased antioxidant capacity
- Increased cellular damage markers
- Documented in studies
Mechanism 2: Organ Overload
The affected organs:
Liver:
- Metabolizes steroids (especially oral steroids)
- Forced to process foreign hormones constantly
- Enzyme systems overworked
- Can lead to liver stress, elevated enzymes, rare cases of liver damage
- Hepatic burden
Kidneys:
- Filter blood, remove waste
- High protein intake + increased muscle mass + steroids = kidney stress
- Increased blood pressure damages nephrons
- Accelerated decline in kidney function
- Renal stress
Heart:
- Enlarged from increased workload (more muscle mass to supply)
- Left ventricular hypertrophy (thickened heart muscle)
- Decreased cardiac efficiency
- Increased risk of arrhythmias and heart failure
- Cardiac remodeling
The resource allocation problem:
- Body diverts resources to damage control
- Less available for normal maintenance and repair
- Both the original function AND damage control suffer
- Unsustainable burden
The result:
- Health problems typical of elderly people
- Appearing in young steroid users
- Premature organ aging and dysfunction
- Accelerated decline
Mechanism 3: Facial Aging and Aesthetic Changes
The visible signs:
Collagen changes:
- Androgens alter collagen production and structure
- Skin becomes thicker but less elastic
- Loss of youthful facial fat distribution
- Harder, more angular features
- Facial structure changes
Accelerated hair loss:
- DHT (dihydrotestosterone) miniaturizes hair follicles
- Androgenic alopecia accelerated dramatically
- Irreversible follicle damage
- Balding pattern of 40-50 year old at age 25-30
- Premature balding
Facial fat redistribution:
- Loss of subcutaneous fat in face
- Hollowed appearance
- Combined with water retention (moon face possible)
- Ages facial appearance 10-15 years
- Aged look
The example:
- Blake Frostad: Bodybuilder at age 22
- Facial appearance of someone 35-40
- Documented transformation visible online
- Visual evidence
Why this matters:
- Face is first thing people see
- Can’t hide facial aging
- Social and psychological impact
- External reflection of internal damage
- Visible marker
Mechanism 4: Cardiovascular Aging
The lipid profile disaster:
LDL increase (bad cholesterol):
- Steroids raise LDL significantly
- Especially oral steroids (drastic effect)
- Promotes arterial plaque formation
- Atherogenic profile
HDL decrease (good cholesterol):
- Protective HDL suppressed
- Can drop to dangerously low levels (<20 mg/dL)
- Removes protective mechanism
- Loss of protection
The result:
- Arterial plaque accumulation accelerated
- Process that normally takes decades happens in years
- Fast-forwarded atherosclerosis
Arterial stiffness:
- Research shows steroid users have arterial stiffness comparable to people 20-30 years older
- Reduced arterial compliance
- Increased cardiovascular stress
- Vascular aging
Blood pressure elevation:
- Common with steroid use
- Chronic hypertension damages organs
- Kidneys, heart, brain all suffer
- Accelerates multiple aging processes
- Hypertensive damage
Heart attack and stroke risk:
- Dramatically elevated compared to non-users
- Can occur in 20s and 30s instead of 60s-70s
- Premature cardiovascular events
The timeline:
- Natural: Cardiovascular disease risk increases 50s-60s
- Steroid abuse: Risk elevated in 20s-30s
- 30-year acceleration
Mechanism 5: Telomere Shortening
What telomeres are:
- Protective caps on the ends of chromosomes
- Like plastic tips on shoelaces
- Prevent DNA damage during cell division
- Chromosomal protection
How telomeres work:
- Each cell division shortens telomeres slightly
- Natural aging process
- When too short, cell can no longer divide
- Cell becomes senescent (inactive) or dies
- Cellular aging clock
How steroids accelerate telomere shortening:
Increased cell division:
- Muscle growth = increased cell division and turnover
- More divisions = faster telomere loss
- Accelerated cellular turnover
Oxidative stress:
- Free radicals damage telomeres directly
- Shortens them beyond normal division-related loss
- Direct damage
The research:
- Some studies suggest chronic supraphysiological hormone exposure accelerates telomere shortening
- Correlates with biological age markers
- Cellular age acceleration
The consequences:
- Reduced cellular regeneration capacity
- Tissues can’t repair as effectively
- Premature cellular senescence
- Biological aging
The timeline:
- Cellular age exceeds chronological age
- 30-year-old with cellular markers of 45-year-old
- Internal age mismatch
Mechanism 6: Brain Aging
The neurological impact:
Oxidative stress in brain:
- Brain highly metabolically active
- Vulnerable to oxidative damage
- Free radicals kill neurons
- Neurons don’t regenerate
- Neuronal loss
Apoptosis (programmed cell death):
- Excessive androgens trigger cell death signals
- Brain cells self-destruct
- Particularly in areas sensitive to hormones
- Accelerated neuronal death
Brain atrophy (shrinkage):
- Key areas physically shrink
- Hippocampus (memory center) reduces in size
- Prefrontal cortex (decision-making) atrophies
- MRI studies document structural changes
- Structural brain changes
BDNF depletion:
- Brain-Derived Neurotrophic Factor
- Critical for neuroplasticity and memory
- Steroid abuse reduces BDNF
- Impairs learning and memory formation
- Cognitive function impairment
The cognitive effects:
- Memory problems
- Reduced executive function
- Impaired decision-making
- Mood dysregulation
- Mental decline
The progression:
- Acute: “Brain fog” during use
- Chronic: Lasting cognitive deficits
- Long-term: Increased dementia risk
- Escalating damage
The research:
- Studies show cognitive testing deficits in long-term users
- Brain imaging reveals structural changes
- Effects can persist after cessation
- Documented impairment
Minimizing Damage (Harm Reduction)
If you insist on using.
Strategy 1: Maintain Healthy Lifestyle Habits
The non-negotiable baseline:
- Don’t smoke (smoking + steroids = disaster)
- Don’t drink excessively (liver already stressed)
- Sleep 7-9 hours nightly (recovery and damage control)
- Manage stress (cortisol + androgens = bad combination)
- Lifestyle foundation
The amplification effect:
- Steroids don’t just add damage to bad habits
- They multiply the consequences
- Bad habit alone: Minor damage
- Bad habit + steroids: Severe damage
- Synergistic harm
The reality check:
- If you can’t maintain healthy habits naturally
- You have no business using steroids
- Steroids punish negligence severely
- Prerequisite discipline
Strategy 2: Strict Dietary Control
Why nutrition matters more:
- Building blocks for cellular repair
- Antioxidant sources
- Inflammation modulation
- Organ support
- Damage control resources
What you need:
- Whole foods (vegetables, fruits, whole grains)
- Quality protein sources
- Anti-inflammatory fats (omega-3s)
- Adequate micronutrients
- Nutrient density
What to avoid:
- Processed foods (inflammatory)
- Excessive saturated fats (already have lipid issues)
- Added sugars (metabolic stress)
- Trans fats (cardiovascular damage)
- Pro-inflammatory foods
The analogy:
- Eating junk + steroids = pouring gasoline on fire
- Optimal nutrition + steroids = damage control
- Food as medicine or poison
The requirement:
- If you can’t follow a meal plan consistently
- Forget about steroids
- Nutrition discipline non-negotiable
- Dietary adherence essential
Strategy 3: Regular Cardiovascular Exercise
Why cardio becomes mandatory:
- Counteracts cardiovascular aging
- Improves lipid profile (slightly)
- Reduces blood pressure
- Enhances arterial health
- Cardiovascular protection
The prescription:
- 150+ minutes moderate cardio weekly
- Or 75+ minutes vigorous
- Mix of steady-state and intervals
- Year-round, not just “cutting”
- Consistent aerobic work
The mistake:
- “Cardio kills gains”
- Bodybuilders skip cardio completely
- Accelerates cardiovascular aging dramatically
- Deadly negligence
The reality:
- For steroid users, cardio isn’t optional
- It’s a survival strategy
- Neglecting cardio = accelerated death
- Life-extending necessity
Strategy 4: Use Minimum Effective Dose
The dose-response relationship:
- More steroids = more gains (to a point)
- Also: More steroids = more damage (linear)
- Diminishing returns meet escalating harm
The math:
- 250mg testosterone/week: Some gains, manageable sides
- 500mg testosterone/week: More gains, more sides
- 1000mg testosterone/week: Marginal additional gains, severe sides
- Returns flatten, damage escalates
The intelligent approach:
- Find minimum dose that produces results
- Don’t exceed it “because more is better”
- Ego lifting with steroids = stupidity
- Conservative dosing
The longevity strategy:
- Lower doses = slower damage accumulation
- More years of use possible (if insisting on using)
- Better health outcomes long-term
- Sustainable approach
Strategy 5: Avoid Trenbolone Specifically
Why trenbolone is the worst:
- Most potent for muscle growth
- Also most damaging for longevity
- Power comes with price
The specific harms:
Severe insomnia:
- Trenbolone notorious for sleep disruption
- Poor sleep impairs oxidative stress management
- Accelerates all aging processes
- Sleep destruction
Cardiovascular damage:
- Particularly harsh on lipids
- HDL crushed, LDL spiked
- Lipid devastation
Neurological effects:
- “Tren rage” (aggression, mood swings)
- Anxiety and paranoia common
- Neurotoxic effects suspected
- Mental health impact
The recommendation:
- Avoid trenbolone entirely if concerned about aging
- Other steroids produce 70-80% of results with 30-40% of damage
- Risk-benefit terrible
Strategy 6: Regular Health Monitoring
Essential bloodwork:
- Lipid panel (LDL, HDL, triglycerides)
- Liver enzymes (AST, ALT)
- Kidney function (creatinine, eGFR)
- Blood pressure monitoring
- Cardiac markers (if long-term user)
- Objective health tracking
The frequency:
- Every 3-6 months minimum
- More often with higher doses or new compounds
- Regular monitoring
The purpose:
- Detect problems early
- Adjust protocols before permanent damage
- Track trends over time
- Early intervention
The reality:
- Many users avoid bloodwork (denial)
- “Ignorance is bliss” until it’s not
- Monitoring allows damage control
- Knowledge enables action
Strategy 7: Plan PCT and Time Off
Post-Cycle Therapy (PCT):
- Restore natural hormone production
- Minimize muscle loss
- Allow body to recover
- Recovery protocol
Time off equals time on (minimum):
- 12-week cycle = 12+ weeks off
- Allows body to reset
- Reduces cumulative damage
- Recovery time
The mistake:
- Blasting and cruising continuously
- Never allowing recovery
- Accelerated damage accumulation
- Constant assault
The wiser approach:
- Cycles with adequate breaks
- Or low-dose TRT between cycles (not high cruise)
- Give body recovery windows
- Periodic respite
TRT vs. Steroid Abuse: The Critical Difference
Understanding the spectrum.
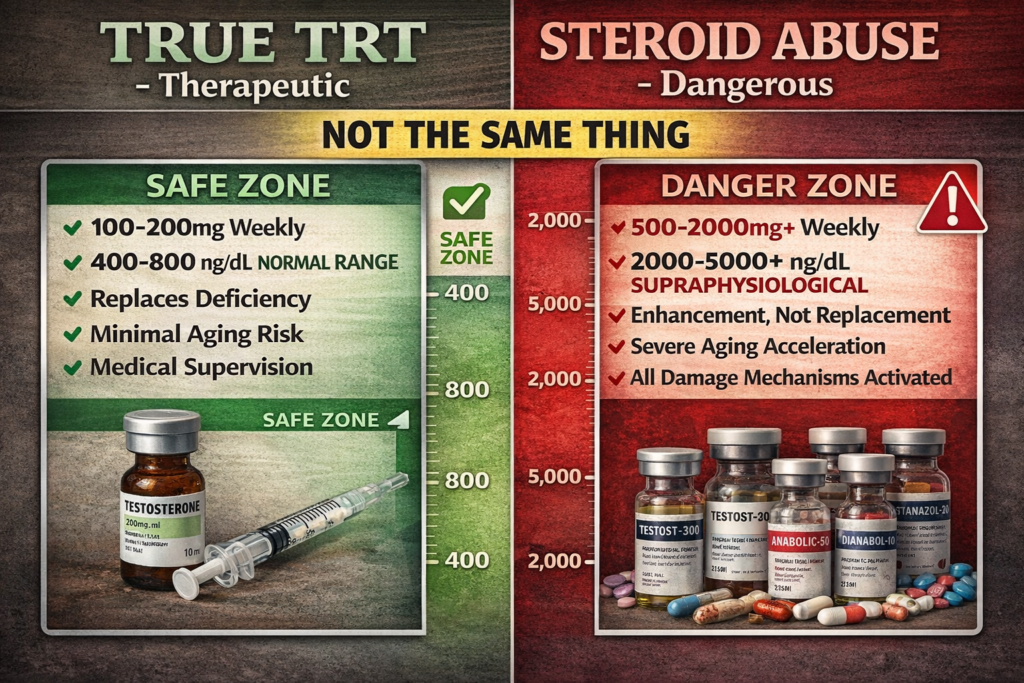
True TRT (Testosterone Replacement Therapy)
The definition:
- Replaces deficient testosterone
- Brings levels into normal physiological range
- Target: 400-800 ng/dL (middle-normal)
- Replacement, not enhancement
Who needs it:
- Men with clinically low testosterone (<300 ng/dL)
- Symptoms of deficiency (fatigue, low libido, muscle loss)
- Diagnosed by physician
- Medical necessity
The dosing:
- Typically 100-200mg testosterone per week
- Maintains normal levels
- No supraphysiological peaks
- Conservative dosing
The effects:
- Restores normal function
- May improve health markers if deficient
- Minimal to no aging acceleration
- Therapeutic benefit
Fake TRT (High-Normal or Supraphysiological)
The problem:
- Some “TRT” clinics prescribe high doses
- Target: 1000-1200 ng/dL (top of range or above)
- Not replacement, it’s enhancement
- Mislabeled abuse
The dosing:
- 200-300mg+ testosterone weekly
- Supraphysiological levels
- Excessive
The consequences:
- Acts more like steroid cycle than TRT
- Aging effects still occur (though less than full abuse)
- Accelerated aging despite “TRT” label
Steroid Abuse (Bodybuilding Doses)
The dosing:
- 500-2000mg+ testosterone per week
- Often stacked with multiple compounds
- Massive supraphysiological doses
The levels:
- Testosterone: 2000-5000+ ng/dL
- 5-10x natural levels
- Extreme elevation
The effects:
- Muscle growth beyond natural limits
- Also: All aging mechanisms activated
- Dose-dependent damage
- Power and poison
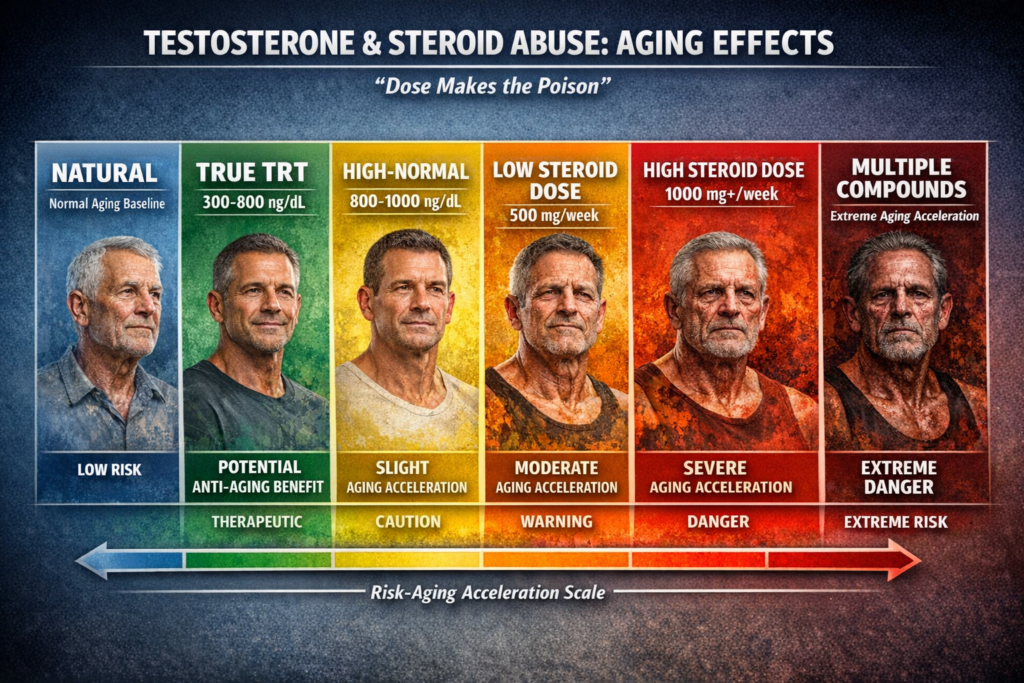
The Spectrum Visualization
The aging risk scale:
- Natural (no TRT): Normal aging
- True TRT (deficient → normal): Potential anti-aging benefit
- High-normal TRT (800-1000 ng/dL): Slight aging acceleration
- Low steroid dose (500mg/week): Moderate aging acceleration
- High steroid dose (1000mg+/week): Severe aging acceleration
- Multiple compounds + high doses: Extreme aging acceleration
- Dose-dependent continuum
FAQ: Common Questions
Addressing specific concerns.
Q1: How long does it take for steroids to accelerate aging?
The answer:
- Damage begins from first use
- Cumulative over time
- Longer use = more permanent damage
- Immediate start, cumulative effect
The timeline:
- Acute effects (cosmetic): Weeks to months
- Cardiovascular changes: Months to years
- Telomere damage: Years to decades
- Variable by mechanism
The individual variation:
- Genetics affect susceptibility
- Some show signs faster (hair loss, facial changes)
- Others accumulate internal damage silently
- Personal variation
Q2: Is steroid-induced aging reversible?
The answer:
- Partially reversible, mostly not
- Mixed outcome
What’s reversible:
- Some lipid profile improvement (after cessation)
- Blood pressure normalization (sometimes)
- Liver enzyme recovery (if no permanent damage)
- Partial cognitive recovery (in some cases)
- Some recovery possible
What’s irreversible:
- Cardiac remodeling (heart enlargement mostly permanent)
- Arterial plaque (doesn’t fully regress)
- Telomere shortening (can’t regrow significantly)
- Hair loss (follicles dead)
- Facial structure changes (bone and collagen remodeling)
- Some brain atrophy (neurons don’t regenerate)
- Permanent damage
The cosmetic options:
- Aesthetic procedures for facial aging
- Hair transplant for baldness
- Can improve appearance but not internal damage
- Surface-level fixes only
Q3: Does TRT cause the same aging as steroids?
The answer:
- True TRT (normal levels): Minimal to no accelerated aging
- Fake TRT (high-normal to super): Some aging effects
- Dose-dependent
The key:
- Staying within natural physiological range is protective
- Going above triggers aging mechanisms
- The threshold matters
The monitoring:
- Even TRT should be monitored
- Ensure levels stay in healthy range
- Adjust if creeping too high
- Medical supervision
Q4: Do women who use steroids age faster than men?
The answer:
- Yes, often more dramatically
- Sex-specific vulnerability
The reasons:
Virilization effects:
- Voice deepening (permanent)
- Facial hair growth (permanent)
- Clitoral enlargement (permanent)
- Facial structure masculinization (permanent)
- Irreversible changes
Hormonal disruption:
- Female body not adapted to high androgens
- More severe metabolic disruption
- Greater impact on appearance
- Increased susceptibility
The aging appearance:
- Can appear decades older rapidly
- Combination of general aging + virilization
- Compounded effects
Q5: Is there a “safe” dose that won’t accelerate aging?
The answer:
- No completely safe supraphysiological dose
- Only risk reduction, not elimination
- Harm reduction, not harm avoidance
The spectrum:
- Lower doses = less damage
- Higher doses = more damage
- But all doses above natural = some damage
- Dose-response relationship
The TRT exception:
- True replacement doses (keeping levels normal): Minimal aging risk
- This is the only “safe” approach
- Replacement vs. enhancement
Q6: Why do some users seem to not age as much?
The factors:
Genetics:
- Some people have superior antioxidant systems
- Better cardiovascular resilience
- More robust telomere protection
- Genetic lottery
Dose and duration:
- Lower doses for shorter time = less damage
- Higher doses for longer = more damage
- Exposure matters
Lifestyle factors:
- Excellent diet, cardio, sleep
- Minimizes damage accumulation
- Harm reduction adherence
The important note:
- Even those who seem fine are still aging faster than if natural
- Just less obvious externally
- Internal damage still occurring
- Hidden costs
The survivor bias:
- The people who aged terribly might have quit or died
- The ones still visible are survivors (for now)
- Selection bias
The Bottom Line: The Price of Unnatural Muscle
After explaining everything:
The truth about steroids and aging:
✅ Supraphysiological steroid doses accelerate aging at cellular and systemic levels (documented mechanisms)
✅ TRT at replacement doses does NOT cause the same effects (normal levels are protective)
✅ Damage is dose-dependent and cumulative (more and longer = worse)
✅ Many aging effects are irreversible (permanent consequences)
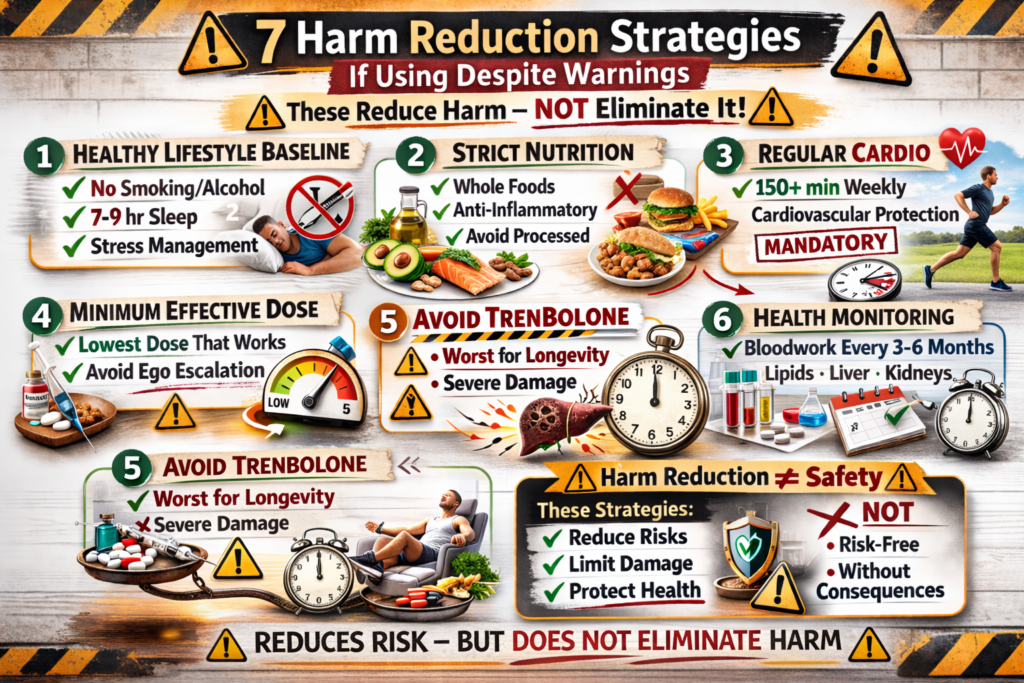
✅ Harm reduction possible but harm elimination not (can reduce but not eliminate risk)
Key takeaways:
The critical quote:
- “Using hormones in the context of hormone replacement (TRT) rejuvenates.”
- “Using more hormones than you need ages you.”
- PhD Gabriel Kaminski
- Dose makes the difference
The aging mechanisms:
1. Oxidative stress:
- Free radical production exceeds clearance
- Cellular machinery damaged (“rust”)
- DNA, proteins, lipids affected
- Widespread cellular damage
2. Organ overload:
- Liver, kidneys, heart stressed beyond capacity
- Resources diverted to damage control
- Premature organ aging and dysfunction
- Health problems of elderly appearing in youth
- Systemic strain
3. Facial aging:
- Collagen alterations (harder, less elastic skin)
- Accelerated hair loss (DHT effects)
- Fat redistribution (hollowed appearance)
- 10-15 year aging appearance
- Visible changes
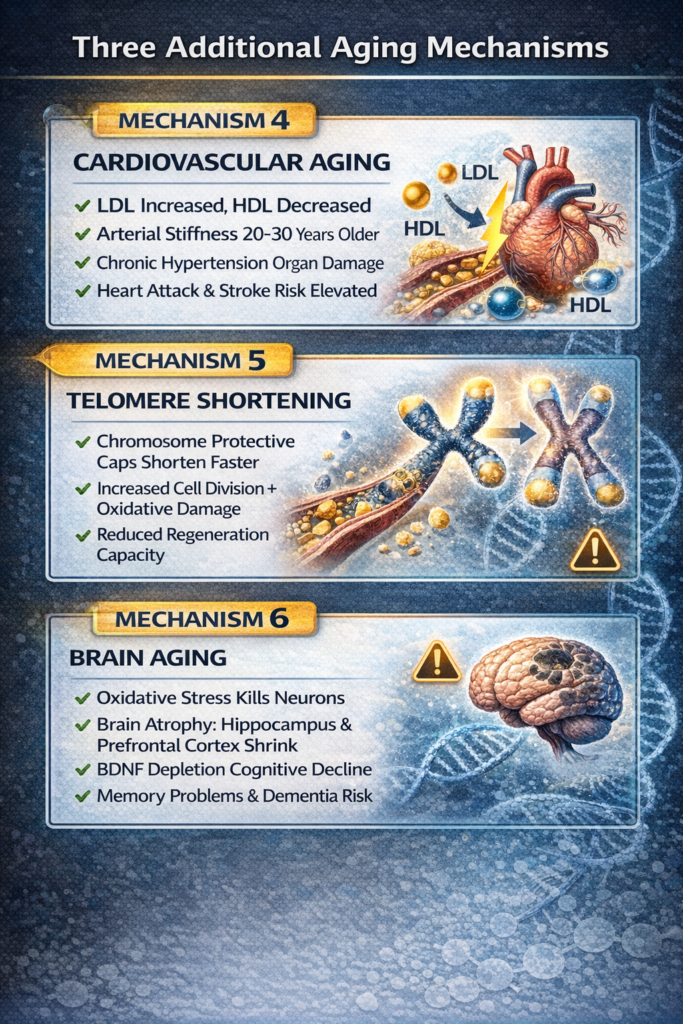
4. Cardiovascular aging:
- LDL increased, HDL decreased (atherogenic profile)
- Arterial stiffness of someone 20-30 years older
- Chronic hypertension (organ damage)
- Dramatically increased heart attack/stroke risk
- Vascular catastrophe
5. Telomere shortening:
- Protective chromosome caps shorten faster
- Increased cell division + oxidative damage
- Reduced regeneration capacity
- Premature cellular senescence
- Biological age acceleration
6. Brain aging:
- Oxidative stress kills neurons
- Programmed cell death (apoptosis)
- Brain atrophy (hippocampus, prefrontal cortex shrink)
- BDNF depletion (impaired neuroplasticity)
- Cognitive decline and dementia risk
- Neurological deterioration
Harm reduction strategies:
1. Healthy lifestyle baseline:
- No smoking, minimal alcohol
- 7-9 hours sleep nightly
- Stress management
- Foundation essential
2. Strict nutrition:
- Whole foods, anti-inflammatory diet
- Adequate micronutrients
- Avoid processed foods
- Dietary discipline
3. Regular cardio:
- 150+ minutes moderate weekly
- Cardiovascular protection
- Not optional, survival strategy
- Mandatory aerobic work
4. Minimum effective dose:
- Lowest dose that produces results
- Avoid ego-driven dose escalation
- Conservative dosing
5. Avoid trenbolone:
- Worst compound for longevity
- Severe insomnia, cardiovascular damage
- Specific avoidance
6. Health monitoring:
- Bloodwork every 3-6 months
- Lipids, liver, kidneys, blood pressure
- Objective tracking
7. Adequate time off:
- Time off equals time on (minimum)
- Allow recovery periods
- Periodic breaks
TRT vs. abuse:
- True TRT (300-800 ng/dL): Minimal aging risk
- Fake TRT (1000+ ng/dL): Some aging acceleration
- Steroid abuse (2000-5000+ ng/dL): Severe aging
- Dose-dependent spectrum
Reversibility:
- Some recovery possible (lipids, blood pressure, partial cognitive)
- Much is irreversible (heart enlargement, arterial damage, telomere loss, hair loss, facial changes, brain atrophy)
- Mostly permanent
Individual variation:
- Genetics affect susceptibility
- Lifestyle modulates damage
- Dose and duration matter
- But everyone ages faster on supraphysiological doses
- Universal effect, variable severity
For women:
- More dramatic aging effects
- Plus irreversible virilization
- Greater vulnerability
NO SAFE SUPRAPHYSIOLOGICAL DOSE. ONLY HARM REDUCTION, NOT ELIMINATION. TRT AT REPLACEMENT LEVELS ≠ STEROID ABUSE. EVERY DOSE ABOVE NATURAL = ACCELERATED AGING. THE PRICE OF UNNATURAL MUSCLE IS PREMATURE AGING.
This article is informational only. We do not condone or recommend steroid use. If considering any hormone therapy, work with qualified medical professionals and understand the serious health risks involved.
REFERENCES
SECTION 1 — The Paradox: TRT vs. Steroid Abuse
[1] Luther PM et al. — Expert Opinion on Pharmacotherapy, 2024 Testosterone replacement therapy: clinical considerations https://pubmed.ncbi.nlm.nih.gov/38229462/
[2] Bhasin S et al. — Journal of Clinical Endocrinology & Metabolism, 2018 Efficacy and Adverse Events of Testosterone Replacement Therapy in Hypogonadal Men: A Systematic Review and Meta-Analysis https://academic.oup.com/jcem/article/103/5/1745/4939466
[3] NIHR Health Technology Assessment Programme, 2024 The effects and safety of testosterone replacement therapy for men with hypogonadism: the TestES evidence synthesis https://pmc.ncbi.nlm.nih.gov/articles/PMC11404359/
SECTION 2 — Mechanism 1: Oxidative Stress
[4] Bezerra de Paiva et al. — Journal of Strength and Conditioning Research, 2017 Use of anabolic androgenic steroids produces greater oxidative stress responses to resistance exercise in strength-trained men https://pubmed.ncbi.nlm.nih.gov/28959650/
[5] Dornelles GL et al. — Molecular and Cellular Biochemistry, 2017 Biochemical and oxidative stress markers in the liver and kidneys of rats submitted to different protocols of anabolic steroids https://pubmed.ncbi.nlm.nih.gov/27896593/
SECTION 3 — Mechanism 4: Cardiovascular Aging
[6] Bjørnstad et al. — Scientific Reports (Nature), 2022 Reduced arterial elasticity after anabolic–androgenic steroid use in young adult males and mice https://www.nature.com/articles/s41598-022-14065-5
[7] Falconi R et al. — European Journal of Preventive Cardiology, 2025 Anabolic steroid abuse accelerates arterial ageing https://academic.oup.com/eurjpc/article/32/Supplement_1/zwaf236.402/8137007
[8] Baggish AL et al. — Circulation / Massachusetts General Hospital Anabolic Steroid Use Linked With Myocardial Dysfunction and Accelerated Atherosclerosis https://www.tctmd.com/news/anabolic-steroid-use-linked-myocardial-dysfunction-and-accelerated-atherosclerosis
[9] Chen Y et al. — World Journal of Cardiology, 2019 Anabolic-androgenic steroids and cardiovascular risk https://pmc.ncbi.nlm.nih.gov/articles/PMC6797160/
[10] Askvik et al. — Scientific Reports (Nature), 2024 Impaired vascular function among young users of anabolic–androgenic steroids https://www.nature.com/articles/s41598-024-70110-5
[11] Bertozzi G et al. — Biomedicines (MDPI), 2025 Anabolic–Androgenic Steroids Induced Cardiomyopathy: A Narrative Review https://www.mdpi.com/2227-9059/13/9/2190
SECTION 4 — Mechanism 6: Brain Aging & Cognitive Decline
[12] Bjørnebekk A et al. — Biological Psychiatry: Cognitive Neuroscience and Neuroimaging, 2021 Long-Term Anabolic-Androgenic Steroid Use Is Associated With Deviant Brain Aging https://pubmed.ncbi.nlm.nih.gov/33811018/
[13] Bjørnebekk A et al. — Biological Psychiatry, 2017 Structural Brain Imaging of Long-Term Anabolic-Androgenic Steroid Users and Nonusing Weightlifters https://www.biologicalpsychiatryjournal.com/article/S0006-3223(16)32529-X/fulltext
[14] Kaufman MJ et al. — Drug and Alcohol Dependence, 2015 Brain and cognition abnormalities in long-term anabolic-androgenic steroid users https://pubmed.ncbi.nlm.nih.gov/25986964/
[15] Salerno M et al. — Brain Sciences (MDPI), 2025 Anabolic–Androgenic Steroids and Brain Damage: A Review of Evidence and Medico-Legal Implications https://www.mdpi.com/2673-6756/5/3/31




Leave a Reply
You must be logged in to post a comment.