Struggling to lose fat despite eating less? Gaining fat easily but can’t build muscle? Your insulin sensitivity is probably broken.
You’re eating in a calorie deficit. You’re training hard. But you’re not losing fat.
Meanwhile, your skinny friend eats pizza and stays lean. You eat one slice and gain weight.
You’ve tried everything:
- Lower calories (just made you hungrier)
- More cardio (exhausting, no results)
- Cutting carbs (temporary results, came back)
- Fat burners (expensive, didn’t work)
Nothing works long-term. You’re metabolically stuck. Your body doesn’t respond like it should.
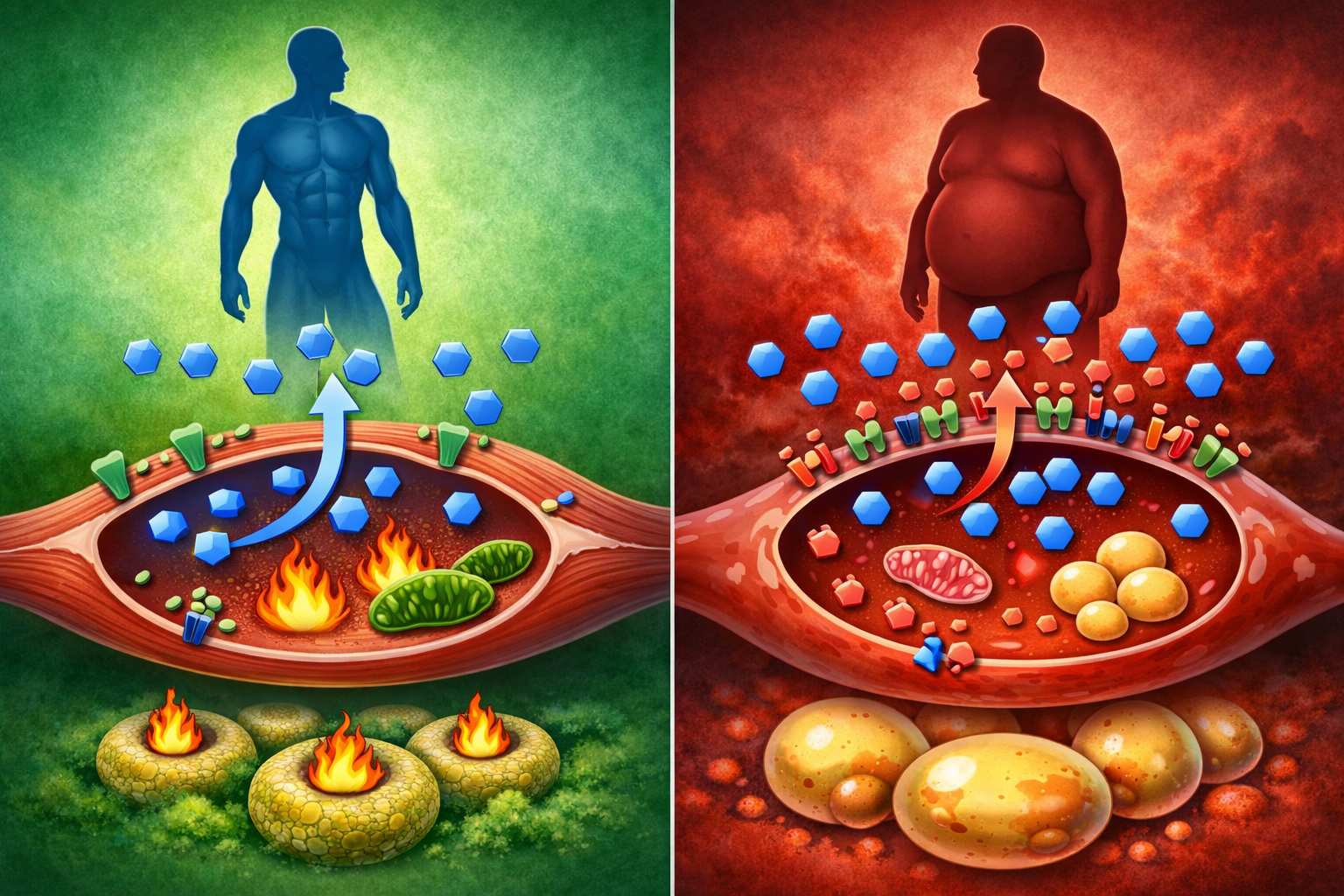
Here’s what’s actually happening: Your cells are insulin resistant. When you eat carbs, your body overproduces insulin to deal with the glucose. High insulin blocks fat burning completely, stores everything as fat, prevents muscle protein synthesis, and makes you constantly hungry. This isn’t about willpower or calories. It’s about hormone signaling. Fix insulin sensitivity, and fat loss becomes effortless while muscle gain accelerates.
In this comprehensive guide, I’ll explain exactly what insulin sensitivity is (and why it’s more important than calories), reveal how insulin resistance develops (most people have some degree), show you the 8 signs you’re insulin resistant (check yourself right now), provide the complete protocol to restore insulin sensitivity (works in 4-8 weeks), and explain why high insulin keeps you fat and weak (the mechanism).
Whether you’re trying to lose stubborn fat, build muscle, or just want better metabolic health, insulin sensitivity is the foundation.
Let’s fix your insulin signaling so your body actually responds to diet and training.
TABLE OF CONTENTS
- Sign 1: Difficulty Losing Fat (Despite Calorie Deficit)
- Sign 2: Fat Gain Around Midsection
- Sign 3: Intense Carb and Sugar Cravings
- Sign 4: Energy Crashes After Meals
- Sign 5: High Triglycerides and Low HDL
- Sign 6: Skin Tags and Darkened Skin
- Sign 7: Frequent Urination and Increased Thirst
- Sign 8: Poor Muscle Building Despite Training
- The Bottom Line: Fix Insulin First
What Is Insulin Sensitivity?
Understanding the most important metabolic variable.
Insulin: The Master Storage Hormone
What insulin does:
- Released by pancreas when you eat carbs
- Signals cells to absorb glucose from bloodstream
- Shuttles glucose into muscle and liver (glycogen storage)
- Promotes protein synthesis (muscle building)
- Inhibits fat breakdown (lipolysis)
- Master regulator of energy storage
The normal process:
- You eat carbohydrates
- Blood glucose rises
- Pancreas releases insulin
- Insulin binds to cell receptors
- Cells open glucose channels
- Glucose enters cells
- Blood glucose normalizes
- Insulin drops back down
- Healthy insulin response
Insulin’s dual role:
Anabolic (building):
- Drives glucose into muscle cells
- Provides energy for workouts
- Promotes protein synthesis
- Builds muscle tissue
- Muscle-building hormone
Anti-lipolytic (fat-storing):
- Stops fat burning completely
- Converts excess glucose to fat
- Stores fat in adipose tissue
- Fat-storage hormone
The key:
- Brief insulin spikes = good (nutrients into muscle)
- Chronically elevated insulin = bad (constant fat storage)
- Timing and magnitude matter
Insulin Sensitivity Explained
What it means:
- How responsive your cells are to insulin
- HIGH sensitivity = cells respond with small insulin amount
- LOW sensitivity = need lots of insulin to get response
- Efficiency of insulin signaling
High insulin sensitivity (good):
- Small insulin release handles glucose
- Glucose goes into muscle, not fat
- Insulin returns to baseline quickly
- Fat burning resumes soon
- Body composition improves
- Metabolically healthy
Low insulin sensitivity / Insulin resistance (bad):
- Pancreas releases lots of insulin
- Cells still don’t respond well
- Glucose stays elevated
- More insulin needed
- Chronically high insulin
- Constant fat storage mode
- Fat loss impossible
- Metabolically broken
The analogy:
- Like volume control on stereo
- Sensitive = whisper produces loud sound (efficient)
- Resistant = shouting barely produces sound (inefficient)
- Signal response efficiency
Why It Matters More Than Calories
Scenario 1: High insulin sensitivity
- Eat 2500 calories with carbs
- Small insulin response
- Glucose goes to muscle
- Insulin drops quickly
- Fat burning resumes
- Maintain or lose fat
- Build muscle
- Efficient metabolism
Scenario 2: Low insulin sensitivity
- Eat 2500 calories with carbs
- Massive insulin response
- Some glucose to muscle, most to fat
- Insulin stays elevated for hours
- No fat burning possible
- Gain fat
- Poor muscle building
- Broken metabolism
Same calories, completely different outcome.
The research:
- Studies show insulin sensitivity predicts:
- Fat loss response to diet
- Muscle gain response to training
- Metabolic health markers
- Longevity
- Better predictor than calorie intake alone
Why most diets fail:
- Focus only on calories
- Ignore insulin sensitivity
- People with poor insulin sensitivity can’t lose fat
- Even in deficit
- Missing the foundation

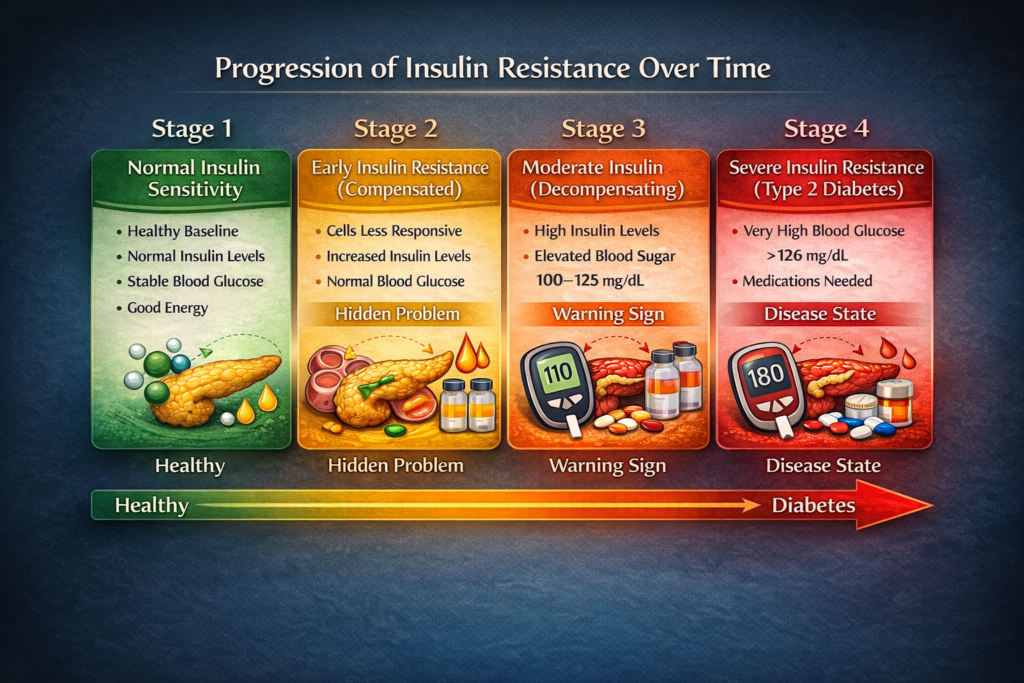
How Insulin Resistance Develops
The progression from healthy to metabolic disaster.
Stage 1: Normal Insulin Sensitivity (Healthy)
Characteristics:
- Eat carbs, moderate insulin release
- Glucose handled efficiently
- Insulin returns to baseline within 2-3 hours
- Energy stable
- Fat loss and muscle gain easy
- Metabolic baseline
Who has this:
- Young, active individuals
- Athletes
- People with healthy lifestyle
- Lean individuals
- The minority in modern society
Stage 2: Early Insulin Resistance (Compensated)
What happens:
- Cells becoming slightly less responsive
- Pancreas compensates by producing more insulin
- Blood glucose still normal (for now)
- Insulin levels elevated (hyperinsulinemia)
- Hidden problem
How it feels:
- Energy crashes after meals
- Cravings 2-3 hours after eating
- Need frequent snacks
- Difficulty losing fat
- Gaining fat more easily
- Subtle symptoms
Lab work:
- Fasting glucose: Normal (70-100 mg/dL)
- Fasting insulin: Elevated (>8-10 μIU/mL)
- HOMA-IR: Elevated (>2.0)
- Problem visible if you test insulin
The danger:
- Most doctors only check glucose
- Glucose still normal at this stage
- Problem not detected
- Continues worsening
- Silent progression
Stage 3: Moderate Insulin Resistance (Decompensating)
What happens:
- Cells very resistant to insulin
- Pancreas struggling to produce enough
- Blood glucose starting to rise
- Insulin very high
- System failing
How it feels:
- Constant fatigue
- Severe carb cravings
- Cannot lose fat
- Easy fat gain
- Poor muscle building
- Brain fog
- Obvious dysfunction
Lab work:
- Fasting glucose: 100-125 mg/dL (pre-diabetic range)
- Fasting insulin: Very high (>15 μIU/mL)
- HOMA-IR: High (>3.0)
- HbA1c: 5.7-6.4% (pre-diabetic)
- Pre-diabetes
The trajectory:
- Without intervention, progresses to diabetes
- Pancreas eventually exhausted
- Can’t produce enough insulin
- Blood sugar out of control
- Heading toward disease
Stage 4: Severe Insulin Resistance / Type 2 Diabetes
What happens:
- Cells extremely resistant
- Pancreas can’t keep up
- Blood glucose chronically elevated
- Medication required
- Disease state
How it feels:
- All previous symptoms amplified
- Neuropathy possible
- Vision problems
- Wound healing issues
- Serious health consequences
Lab work:
- Fasting glucose: >126 mg/dL
- HbA1c: >6.5%
- Type 2 diabetes diagnosis
- Disease diagnosis
What Causes Insulin Resistance?
The primary drivers:
Cause 1: Chronic carbohydrate overconsumption
- Eating carbs constantly
- Insulin always elevated
- Cells exposed to insulin 24/7
- Receptors downregulate
- Become desensitized
- Like turning down volume on alarm
Mechanism:
- Constant stimulus
- Cells protect themselves from constant signal
- Reduce receptor number
- Reduce receptor sensitivity
- Adaptive response
Cause 2: Excessive body fat (especially visceral)
- Fat cells produce inflammatory signals
- Cytokines (TNF-alpha, IL-6)
- These directly impair insulin signaling
- More fat = more inflammation = worse insulin sensitivity
- Visceral fat most problematic
The vicious cycle:
- Insulin resistance → fat gain (especially visceral)
- More visceral fat → worse insulin resistance
- Self-perpetuating
Cause 3: Physical inactivity
- Muscle is primary glucose disposal site
- Inactive muscle = reduced glucose uptake
- Exercise improves insulin sensitivity immediately
- Sedentary lifestyle progressively worsens it
- Use it or lose it
Mechanism:
- Muscle contraction activates GLUT4 transporters
- Independent of insulin
- Exercise improves insulin signaling pathways
- Inactivity causes them to atrophy
- Activity essential
Cause 4: Poor sleep
- Even one night of poor sleep reduces insulin sensitivity 20-30%
- Chronic poor sleep major contributor
- Affects glucose metabolism directly
- Sleep disruption = metabolic disruption
Research:
- 4 hours sleep vs. 8 hours
- 30% reduction in insulin sensitivity
- One night
- Massive acute impact
Cause 5: Chronic stress
- Elevated cortisol increases blood glucose
- Insulin must rise to compensate
- Chronic elevation drives resistance
- Stress-metabolic connection
Cause 6: Genetics
- Some people more susceptible
- Family history matters
- Ethnicity matters (South Asian, Hispanic higher risk)
- But lifestyle still primary driver
- Predisposition, not destiny
Cause 7: Aging
- Insulin sensitivity naturally declines with age
- Muscle mass loss
- Fat gain
- Reduced activity
- Lifestyle factors accelerate
Cause 8: Poor diet quality
- Processed foods
- Trans fats
- Excess omega-6 fatty acids
- Low fiber
- Inflammatory diet
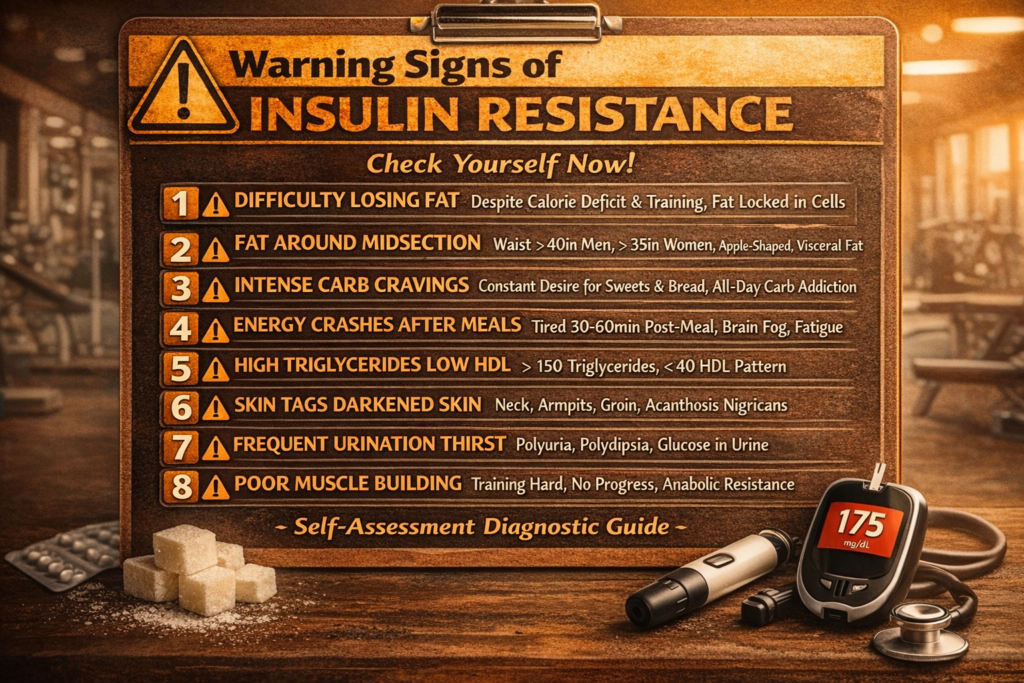
8 Signs You’re Insulin Resistant
Check yourself right now.
Sign 1: Difficulty Losing Fat (Despite Calorie Deficit)
What happens:
- Eating in deficit
- Training regularly
- Scale won’t budge
- Body composition not improving
- Frustrating plateau
Why:
- Insulin constantly elevated
- Blocks lipolysis (fat breakdown)
- Can’t access fat stores
- Even with calorie deficit
- Fat locked in cells
The test:
- If you’re in verified calorie deficit
- Training consistently
- Not losing fat after 4+ weeks
- Likely insulin resistant
- Strong indicator
Sign 2: Fat Gain Around Midsection
What happens:
- Fat accumulates around waist
- Apple-shaped body
- Visceral fat (around organs)
- Even if extremities relatively lean
- Central adiposity
Why:
- High insulin preferentially stores fat in abdomen
- Visceral adipose tissue most insulin-sensitive
- First place fat goes with high insulin
- Insulin’s favorite storage site
The measurement:
- Waist circumference
- Men: >40 inches (102 cm) concerning
- Women: >35 inches (88 cm) concerning
- Waist-to-hip ratio
- Simple home assessment
Sign 3: Intense Carb and Sugar Cravings
What happens:
- Constant desire for sweets, bread, pasta
- Feel like you NEED carbs
- Can’t stop at one serving
- Especially crave in afternoon
- Uncontrollable urges
Why:
- Blood sugar rollercoaster
- Eat carbs → insulin spike → blood sugar crash
- Crash triggers intense craving
- Cycle repeats
- Reactive hypoglycemia
The pattern:
- Breakfast carbs (cereal, toast)
- Hungry 2 hours later
- Snack on carbs
- Lunch with carbs
- Afternoon crash, need carbs
- All-day carb addiction
Sign 4: Energy Crashes After Meals
What happens:
- Eat meal, especially carb-heavy
- Feel tired 30-60 minutes later
- Need to nap
- Brain fog sets in
- Post-meal fatigue
Why:
- Large insulin spike
- Glucose drops too low (overcompensation)
- Brain lacks fuel
- Body redirecting blood flow to digestion
- Exaggerated response
The normal response:
- Should feel satisfied and energized after eating
- Not exhausted
- Stable energy
- Meals should fuel you, not drain you
Sign 5: High Triglycerides and Low HDL
What happens:
- Blood test shows:
- Triglycerides >150 mg/dL
- HDL <40 mg/dL (men) or <50 mg/dL (women)
- Classic insulin resistance pattern
- Lipid dysfunction
Why:
- High insulin promotes fat synthesis in liver
- Creates VLDL particles (become triglycerides)
- Suppresses HDL production
- Insulin-driven dyslipidemia
The significance:
- Even if total cholesterol “normal”
- This pattern indicates insulin resistance
- Cardiovascular risk
- Important marker
Sign 6: Skin Tags and Darkened Skin
What happens:
- Small skin tags (acrochordons)
- Especially neck, armpits, groin
- Dark, velvety patches (acanthosis nigricans)
- Neck, armpits, groin
- Physical manifestations
Why:
- High insulin stimulates skin cell growth
- Creates skin tags
- Insulin affects pigmentation
- Darkened patches
- Visible insulin excess
The indicator:
- Not everyone with skin tags has insulin resistance
- But most people with insulin resistance develop them
- Useful visual indicator
- Physical sign
Sign 7: Frequent Urination and Increased Thirst
What happens:
- Need to urinate frequently
- Excessive thirst
- Especially noticeable at night
- Polyuria and polydipsia
Why:
- If blood glucose elevated (even mildly)
- Kidneys trying to excrete excess glucose
- Pulls water with it
- Leads to dehydration and thirst
- Body trying to normalize glucose
Important:
- If severe, see doctor immediately
- Could be diabetes
- Not just insulin resistance
- Medical evaluation needed
Sign 8: Poor Muscle Building Despite Training
What happens:
- Training consistently
- Eating adequate protein
- Not building muscle
- Looking “soft” despite training
- No progress
Why:
- Insulin resistance impairs protein synthesis signaling
- mTOR pathway disrupted
- Amino acids don’t enter muscle efficiently
- Can’t build muscle properly
- Anabolic resistance
The frustration:
- Doing everything “right”
- No results
- Insulin resistance undermining efforts
- Hidden saboteur
How to Test Your Insulin Sensitivity
Proper assessment methods.
Lab Tests (Most Accurate)
Fasting insulin:
- Single best marker
- Cheap, simple blood test
- Optimal: <5 μIU/mL
- Good: 5-8 μIU/mL
- Borderline: 8-12 μIU/mL
- Concerning: >12 μIU/mL
- Must be fasted (8-12 hours)
Fasting glucose:
- Standard test doctors order
- But not sensitive enough alone
- Optimal: 70-85 mg/dL
- Good: 85-95 mg/dL
- Borderline: 95-100 mg/dL
- Pre-diabetic: 100-125 mg/dL
- Can be normal with insulin resistance
HOMA-IR (calculated):
- Homeostatic Model Assessment of Insulin Resistance
- Formula: (Fasting Glucose × Fasting Insulin) / 405
- Optimal: <1.0
- Good: 1.0-1.5
- Borderline: 1.5-2.5
- Insulin resistant: >2.5
- Combines glucose and insulin
HbA1c:
- Average blood glucose over 3 months
- Optimal: <5.0%
- Good: 5.0-5.6%
- Pre-diabetic: 5.7-6.4%
- Diabetic: ≥6.5%
- Long-term marker
Lipid panel:
- Triglycerides
- HDL
- Pattern:
- Triglycerides >150 + HDL <40 = likely insulin resistant
- Triglycerides <100 + HDL >60 = likely insulin sensitive
- Secondary marker
The ideal panel:
- Fasting glucose
- Fasting insulin (CRITICAL)
- HbA1c
- Lipid panel
- Calculate HOMA-IR
At-Home Assessments (Less Accurate)
Continuous glucose monitor (CGM):
- Wearable sensor
- Tracks glucose 24/7
- See response to meals
- Identify problematic foods
- Very informative but expensive
What to look for:
- Post-meal glucose spike <30-40 mg/dL
- Return to baseline within 2 hours
- Fasting glucose 70-90 mg/dL
- Stable overnight
- Healthy patterns
Waist measurement:
- Measure around belly button
- Men: <37 inches ideal, <40 acceptable
- Women: <31 inches ideal, <35 acceptable
- Increasing waist = worsening insulin sensitivity
- Simple tracking
Symptom tracking:
- Energy after meals
- Cravings frequency
- Sleep quality
- Training performance
- Subjective but useful
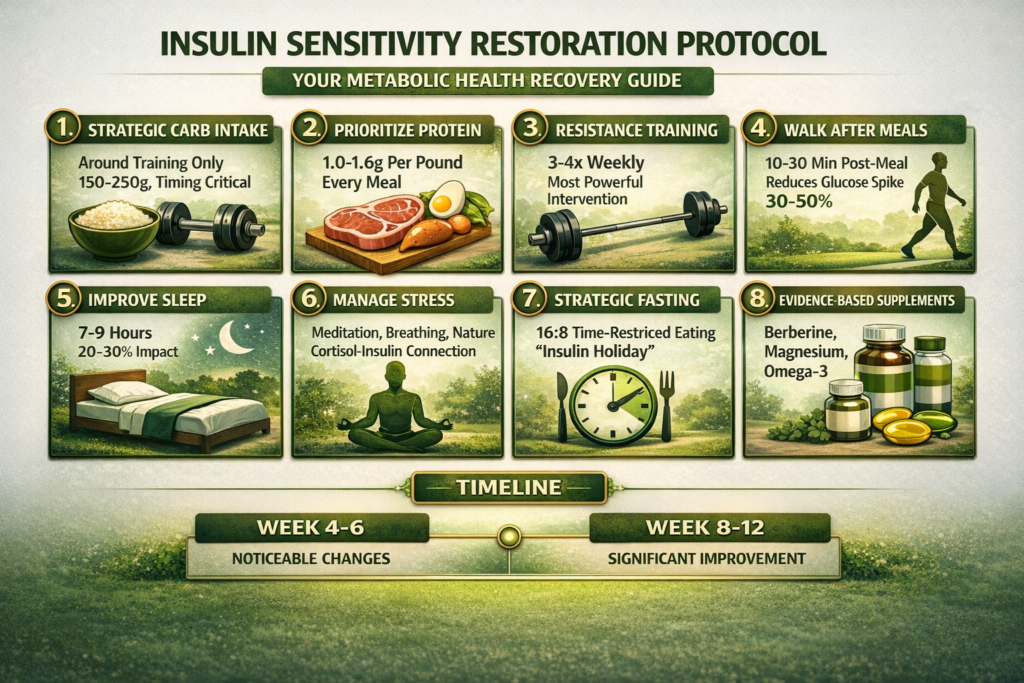
The Complete Protocol to Restore Insulin Sensitivity
Evidence-based strategies that work.
Strategy 1: Strategic Carbohydrate Intake
Why it works:
- Reducing carb frequency lowers insulin exposure
- Cells regain sensitivity
- Like letting ears rest from loud noise
- Reduces constant stimulus
The approach:
Carb timing (most important):
- Eat carbs around training only
- Pre-workout: 1-2 hours before (fuel)
- Post-workout: Within 2 hours after (recovery)
- Other meals: Protein and fat based
- Time carbs strategically
Example day (training at 5 PM):
- Breakfast (8 AM): 4 eggs, avocado, vegetables (no carbs)
- Lunch (12 PM): Chicken, salad, olive oil (no carbs)
- Pre-workout (3:30 PM): Rice, chicken (carbs here)
- Post-workout (6:30 PM): Potato, steak, vegetables (carbs here)
- Carbs only around training
Carb amount:
- Training days: 150-250g (around workouts)
- Rest days: <100g (optional, can be zero)
- Adjust based on activity and size
- Matched to activity
Carb types:
- Prioritize: Rice, potatoes, oats, fruit
- Minimize: Bread, pasta, processed foods
- Whole food sources
- Quality matters
Why this works:
- Insulin only elevated briefly
- Glucose goes to muscle (insulin-independent during/after training)
- Long periods of low insulin (fat burning)
- Cells resensitize
- Strategic exposure
Strategy 2: Prioritize Protein
Why it works:
- Protein most satiating macronutrient
- Minimal insulin response compared to carbs
- Preserves muscle during fat loss
- Supports muscle building
- Foundation macronutrient
The protocol:
- 1.0g per pound body weight minimum
- 1.2-1.6g per pound ideal for athletes
- Every meal includes protein
- Non-negotiable
Distribution:
- 30-50g per meal (4 meals = 120-200g total for 150lb person)
- Protein at breakfast critical
- Evening protein supports overnight recovery
- Spread throughout day
Best sources:
- Lean meats (chicken, turkey, lean beef)
- Fish (salmon, cod, tuna)
- Eggs
- Greek yogurt
- Whey protein
- High-quality protein
Strategy 3: Resistance Training (Most Powerful)
Why it’s critical:
- Single most effective insulin sensitivity intervention
- Muscle contraction activates glucose uptake independent of insulin
- Builds muscle (more glucose disposal capacity)
- Effects last 24-48 hours post-workout
- Unmatched effectiveness
The research:
- One training session improves insulin sensitivity for 24-72 hours
- Regular training produces chronic improvements
- More effective than cardio
- Evidence overwhelming
The protocol:
Frequency:
- 3-4 times per week minimum
- Full body or upper/lower split
- Consistency matters most
Exercise selection:
- Compound movements (use most muscle)
- Squats, deadlifts, bench press, rows
- Machines acceptable
- Big movements
Volume:
- 10-20 sets per muscle group per week
- 6-15 reps per set
- Progressive overload
- Adequate stimulus
Why it works:
- Depletes muscle glycogen (makes room for more glucose)
- Increases GLUT4 transporters in muscle
- Builds muscle mass (more glucose disposal)
- Improves insulin signaling pathways
- Multiple mechanisms
Strategy 4: Walking After Meals
Why it works:
- Muscles use glucose when contracting
- Lowers post-meal glucose spike
- Reduces insulin needed
- Simple and sustainable
- Easy intervention
The protocol:
- 10-30 minute walk after meals
- Especially after carb-containing meals
- Moderate pace (3-4 mph)
- Immediately after eating
The research:
- 15-minute walk after meals
- Reduces glucose spike by 30-50%
- Significant insulin sensitivity improvement
- Well-documented benefit
Practical implementation:
- After dinner (easiest to implement)
- After lunch if possible
- Morning walk if fasted breakfast
- Build into routine
Strategy 5: Improve Sleep Quality
Why it’s critical:
- Sleep deprivation reduces insulin sensitivity by 20-30%
- One bad night has immediate effect
- Chronic poor sleep major contributor
- Non-negotiable
The protocol:
- 7-9 hours nightly (minimum 7)
- Consistent schedule (same bedtime/wake)
- Dark room (blackout curtains)
- Cool temperature (65-68°F)
- No screens 1 hour before bed
- Sleep hygiene essentials
If struggling:
- Magnesium glycinate (400mg before bed)
- Avoid caffeine after 2 PM
- No alcohol (disrupts sleep quality)
- Consider sleep study if suspected apnea
- Address aggressively
Strategy 6: Manage Stress
Why it matters:
- Chronic stress elevates cortisol
- Cortisol increases blood glucose
- More insulin needed
- Drives insulin resistance
- Stress-metabolic connection
The approach:
Daily practices:
- Meditation (10-20 minutes)
- Deep breathing (5-10 minutes, 2-3x daily)
- Nature exposure (20-30 minutes)
- Social connection
- Stress reduction
Lifestyle:
- Identify and address major stressors
- Set boundaries
- Adequate rest days (don’t overtrain)
- Enjoyable activities
- Holistic approach
Strategy 7: Strategic Fasting
Why it works:
- No food = no insulin
- Allows insulin to drop to baseline
- Cells regain sensitivity
- Fat burning occurs
- Insulin holiday
The approach:
Time-restricted eating (most sustainable):
- 8-hour eating window
- 16-hour fast
- Example: Eat 12 PM – 8 PM
- Fast 8 PM – 12 PM next day
- Daily rhythm
Benefits:
- Extends overnight fast
- Reduces insulin exposure
- Improves insulin sensitivity
- Fat loss enhanced
- Simple to implement
Important notes:
- Not for everyone
- If training early, may need breakfast
- Listen to body
- Individual response
What NOT to do:
- Extended fasts (24+ hours) repeatedly
- Can increase cortisol
- May impair training
- Not necessary
- Moderate approach
Strategy 8: Specific Supplements
Evidence-based only:
Tier 1: Strong evidence
Berberine:
- 500mg, 3x daily with meals
- Activates AMPK (similar to metformin)
- Improves glucose uptake
- Reduces liver glucose production
- Comparable to medication
Magnesium:
- 400mg daily
- Cofactor in insulin signaling
- Most people deficient
- Glycinate form best
- Foundation supplement
Omega-3 fish oil:
- 2-3g EPA+DHA daily
- Reduces inflammation
- Improves insulin signaling
- Anti-inflammatory
Tier 2: Moderate evidence
Alpha-lipoic acid:
- 300-600mg daily
- Improves glucose uptake
- Antioxidant
- May help
Chromium picolinate:
- 200-400mcg daily
- Enhances insulin function
- Mixed evidence
- Modest benefit
Cinnamon:
- 1-6g daily
- May improve insulin sensitivity
- Food source fine
- Minor effect
What doesn’t work:
- Most “glucose disposal agents”
- Expensive proprietary formulas
- Unproven compounds
- Save money
Timeline for Improvement
What to expect:
Week 1:
- Implementing changes
- May feel tired initially (carb adaptation)
- Cravings may increase temporarily
- Adjustment period
Week 2-3:
- Energy stabilizing
- Cravings reducing
- Sleep improving
- Early improvements
Week 4-6:
- Noticeable energy increase
- Fat loss beginning
- Strength increasing
- Body composition changing
- Visible progress
Week 8-12:
- Significant insulin sensitivity improvement
- Fat loss accelerating
- Muscle building improving
- Metabolic health transforming
- Major changes
Month 3-6:
- Full restoration possible (if caught early)
- New baseline established
- Body composition dramatically improved
- Long-term success
The reality:
- Degree of resistance determines timeline
- Worse starting point = longer recovery
- But improvement begins immediately
- Consistency is everything
- Patience required
Why High Insulin Keeps You Fat and Weak
The mechanisms explained.
How Insulin Blocks Fat Loss
Mechanism 1: Direct inhibition of lipolysis
- Insulin suppresses hormone-sensitive lipase (HSL)
- HSL breaks down stored fat (triglycerides)
- No HSL = no fat breakdown
- Fat locked in adipose tissue
- Can’t access fat stores
The effect:
- Even in calorie deficit
- If insulin elevated
- Body can’t release fat
- Burns muscle instead
- Preferential muscle loss
Mechanism 2: Promotes fat storage
- Insulin activates lipoprotein lipase (LPL)
- LPL takes fat from blood into fat cells
- More insulin = more fat storage
- Especially in visceral area
- Fat accumulation
Mechanism 3: Converts glucose to fat
- Excess glucose (can’t fit in muscle/liver)
- Converted to fat via de novo lipogenesis
- High insulin promotes this process
- New fat created from carbs
- Carbs become fat
The practical implication:
- Carb-heavy meal
- Insulin spike for 2-4 hours
- During this time: Zero fat burning
- 3 carb meals = 6-12 hours no fat burning
- Constant carbs = 24/7 fat storage
- Insulin timeline matters
How Insulin Resistance Prevents Muscle Building
Mechanism 1: Impaired nutrient partitioning
- Insulin should drive nutrients into muscle
- With resistance, goes to fat instead
- Amino acids → fat cells, not muscle
- Glucose → fat cells, not muscle
- Wrong destination
Mechanism 2: Impaired mTOR activation
- mTOR (mechanistic target of rapamycin)
- Master regulator of protein synthesis
- Insulin activates mTOR
- Insulin resistance impairs this activation
- Less muscle protein synthesis
- Anabolic signaling blocked
Mechanism 3: Chronic inflammation
- Insulin resistance creates inflammatory state
- Inflammation directly impairs protein synthesis
- Increases protein breakdown
- Net result: muscle loss
- Inflammatory muscle wasting
Mechanism 4: Energy partitioning
- Limited glucose getting into muscle
- Less glycogen storage
- Poor workout fuel
- Reduced training stimulus
- Poor performance
The practical implication:
- Can train hard
- Eat adequate protein
- But insulin resistance prevents growth
- Spinning wheels
- Fix insulin first

Insulin Sensitivity and Body Recomposition
Why it’s the key to simultaneous fat loss and muscle gain.
Why Body Recomposition Requires Good Insulin Sensitivity
The nutrient partitioning effect:
With good insulin sensitivity:
- Carbs → muscle glycogen (fuel)
- Protein → muscle tissue (building)
- Fat → energy between meals
- Optimal partitioning
With insulin resistance:
- Carbs → fat storage
- Protein → fat storage or wasted
- Fat → stored, not burned
- Poor partitioning
The research:
- Insulin sensitivity predicts body recomposition success
- Better sensitivity = more muscle gain + more fat loss simultaneously
- Poor sensitivity = choose one or the other (can’t do both)
- Foundation for recomp
The Recomp Protocol
Prerequisites:
- Restore insulin sensitivity first (8-12 weeks)
- THEN attempt recomp
- Won’t work with poor insulin sensitivity
- Foundation required
The approach:
Calories:
- Slight deficit (-200-300 calories)
- Or maintenance
- Not aggressive deficit
- Modest restriction
Protein:
- Very high (1.2-1.6g per pound)
- Supports muscle building in deficit
- Maximized protein
Carbs:
- Around training only
- 150-250g on training days
- <100g on rest days
- Strategic timing
Training:
- Progressive resistance training 4-5x weekly
- Adequate volume (15-20 sets per muscle per week)
- Focus on strength progression
- Stimulus for growth
Why it works (with good insulin sensitivity):
- Post-workout: Insulin high, nutrients to muscle
- Between meals: Insulin low, fat burning
- Net result: Lose fat + gain muscle
- Optimal partitioning
The Bottom Line: Fix Insulin First
After explaining everything:
The truth about insulin sensitivity:
✅ More important than calorie counting (determines nutrient partitioning)
✅ Determines whether you lose fat or stay stuck (high insulin blocks lipolysis)
✅ Determines whether you build muscle or waste protein (affects anabolic signaling)
✅ Can be restored in 8-12 weeks (with proper protocol)
✅ Foundation of metabolic health (affects everything)
Key takeaways:
What insulin sensitivity is:
- How well cells respond to insulin
- High sensitivity = efficient glucose disposal, muscle building, fat burning
- Low sensitivity / resistance = fat storage, poor muscle building, metabolic dysfunction
- Master metabolic variable
How insulin resistance develops:
- Chronic carb overconsumption (constant insulin exposure)
- Excess body fat (inflammation)
- Physical inactivity (muscles not using glucose)
- Poor sleep (30% reduction from one bad night)
- Chronic stress (cortisol-insulin interaction)
- Genetics and aging (predisposition)
- Multiple contributing factors
8 signs you’re insulin resistant:
- Can’t lose fat despite deficit
- Fat accumulation around midsection
- Intense carb and sugar cravings
- Energy crashes after meals
- High triglycerides and low HDL
- Skin tags and darkened skin patches
- Frequent urination and increased thirst
- Poor muscle building despite training
- Check yourself
How to test:
- Best: Fasting insulin (<5 μIU/mL optimal)
- Calculate HOMA-IR (<1.0 optimal)
- HbA1c (<5.0% optimal)
- Lipid panel (triglycerides <100, HDL >60)
- Proper lab work essential
The complete protocol:
- Strategic carb intake (around training only, 150-250g training days)
- Prioritize protein (1.0-1.6g per pound daily)
- Resistance training (3-4x weekly, compound movements)
- Walk after meals (10-30 minutes, especially after carbs)
- Optimize sleep (7-9 hours nightly)
- Manage stress (meditation, breathing, nature)
- Strategic fasting (16:8 time-restricted eating)
- Evidence-based supplements (berberine, magnesium, omega-3)
- Complete approach
Timeline:
- Week 1: Adjustment period
- Week 2-3: Early improvements
- Week 4-6: Noticeable changes
- Week 8-12: Significant improvement
- Month 3-6: Full restoration possible
- Requires consistency
Why high insulin keeps you fat:
- Directly blocks fat breakdown (inhibits HSL)
- Promotes fat storage (activates LPL)
- Converts excess glucose to fat (de novo lipogenesis)
- Carb-heavy meals = hours of fat storage mode
- Mechanism clear
Why insulin resistance prevents muscle building:
- Poor nutrient partitioning (nutrients to fat, not muscle)
- Impaired mTOR activation (less protein synthesis)
- Chronic inflammation (increases breakdown)
- Poor workout fuel (limited muscle glycogen)
- Multiple mechanisms
Body recomposition:
- Requires good insulin sensitivity first
- Can’t happen with insulin resistance
- Restore sensitivity, then attempt recomp
- Foundation essential
Priority actions:
- Get fasting insulin tested (not just glucose)
- Implement strategic carb timing (training only)
- Start resistance training (non-negotiable)
- Fix sleep immediately (7+ hours)
- Walk after meals (easiest quick win)
- Start now
FIX INSULIN SENSITIVITY FIRST. EVERYTHING ELSE BECOMES EASIER.
Ready to build a complete metabolic optimization system with proper insulin sensitivity testing, strategic nutrition timing, progressive training protocols, and lifestyle strategies that transform your body composition while improving long-term health? Understanding insulin is just the beginning. Get a comprehensive guide to restoring insulin sensitivity completely, optimizing nutrient partitioning, building muscle while losing fat simultaneously, and achieving the physique you want without fighting your biology. Stop fighting insulin. Start working with it to achieve effortless results.
REFERENCES
SECTION 1 — How Insulin Resistance Develops (Visceral Fat → Inflammation)
[1] Hotamisligil GS et al. — Science, 1996 IRS-1-mediated inhibition of insulin receptor tyrosine kinase activity in TNF-alpha- and obesity-induced insulin resistance https://pubmed.ncbi.nlm.nih.gov/15146098/
[2] Cancello R, Clément K. — Journal of Internal Medicine, 2006 Visceral obesity and plasma glucose-insulin homeostasis: contributions of IL-6 and TNF-alpha https://pubmed.ncbi.nlm.nih.gov/18319319/
SECTION 2 — How Insulin Blocks Fat Loss (HSL Mechanism)
[3] Girousse A et al. — PLoS Biology, 2013 Partial inhibition of adipose tissue lipolysis improves glucose metabolism and insulin sensitivity https://pubmed.ncbi.nlm.nih.gov/23431266/
[4] Zhao L et al. — Frontiers in Endocrinology, 2019 Update on the synergistic effect of HSL and insulin in the treatment of metabolic disorders (review of insulin’s inhibition of HSL/lipolysis pathway) https://pubmed.ncbi.nlm.nih.gov/31565213/
SECTION 3 — Resistance Training Improves Insulin Sensitivity (GLUT4)
[5] Koopman R et al. — European Journal of Applied Physiology, 2005 A single session of resistance exercise enhances insulin sensitivity for at least 24 h in healthy men https://pubmed.ncbi.nlm.nih.gov/15761746/
[6] Bird SR, Hawley JA. — BMJ Open Sport & Exercise Medicine, 2017 The acute vs. chronic effect of exercise on insulin sensitivity — effect lasts up to 72 hours https://pmc.ncbi.nlm.nih.gov/articles/PMC8352615/
[7] Dela F et al. — Diabetes, 2004 Strength training increases insulin-mediated glucose uptake, GLUT4 content, and insulin signaling in skeletal muscle in patients with type 2 diabetes https://pubmed.ncbi.nlm.nih.gov/14747278/
SECTION 4 — Walking After Meals Lowers Glucose Spike
[8] Hashimoto K et al. — Scientific Reports, 2025 Positive impact of a 10-min walk immediately after glucose intake on postprandial glucose levels (randomized crossover trial) https://pubmed.ncbi.nlm.nih.gov/40594496/
[9] DiPietro L et al. — Diabetes Care, 2013 Three 15-min bouts of moderate postmeal walking significantly improves 24-h glycemic control in older people at risk for impaired glucose tolerance https://diabetesjournals.org/care/article/36/10/3262/30770/
SECTION 5 — Poor Sleep Reduces Insulin Sensitivity
[10] Donga E et al. — Diabetes, 2010 Sleep Restriction for 1 Week Reduces Insulin Sensitivity in Healthy Men (euglycemic clamp study) https://pubmed.ncbi.nlm.nih.gov/20622169/
[11] Brady M (University of Chicago) — Annals of Internal Medicine, 2012 4 nights of restricted sleep (4.5h): total-body insulin response decreased 16%, fat cell insulin sensitivity decreased 30% https://www.acponline.org/acp-newsroom/short-term-sleep-deprivation-significantly-decreases-insulin-sensitivity-in-fat-cells
SECTION 6 — Berberine Comparable to Metformin
[12] Zhang Y et al. — Metabolism, 2008 Efficacy of berberine in patients with type 2 diabetes mellitus — hypoglycemic effect comparable to metformin, HOMA-IR reduced 44.7% https://pubmed.ncbi.nlm.nih.gov/18442638/
[13] Liang Y et al. — Frontiers in Pharmacology, 2019 Metformin and berberine, two versatile drugs in treatment of common metabolic diseases — both activate AMPK through similar pathways https://pmc.ncbi.nlm.nih.gov/articles/PMC5839379/






Leave a Reply
You must be logged in to post a comment.