
Using Sustanon and confused about injection frequency? The half-life determines everything: dosing schedule, PCT timing, and how long it stays in your system.
You inject Sustanon. You wonder when to inject again. Some say once a week. Others say every 3 weeks.
The confusion comes from Sustanon containing 4 different testosterone esters with different half-lives. Most people don’t understand which one actually matters.
You’ve heard:
- “Inject once weekly” (some users)
- “Inject every 2 weeks” (some doctors)
- “Inject twice weekly for stable levels” (other users)
- “All four esters matter equally” (wrong)
The truth: Sustanon’s half-life is 15-20 days, determined by its longest ester (testosterone decanoate). This single ester dictates injection frequency, PCT timing, and system clearance time. The other three esters (propionate, phenylpropionate, isocaproate) clear much faster but are irrelevant for half-life calculations. Understanding this prevents hormone fluctuations, premature PCT, and prolonged side effects.
In this comprehensive guide, I’ll explain what half-life actually means (the pharmacokinetic concept), reveal Sustanon’s 4-ester composition (and why only the longest matters), show you optimal injection frequency (weekly vs. bi-weekly protocols), provide PCT timing guidelines (when to actually start), and calculate complete system clearance (the 5 half-life rule).
Whether you’re using Sustanon for TRT or performance enhancement, understanding half-life is fundamental.
Let’s break down Sustanon pharmacokinetics precisely.
TABLE OF CONTENTS
- Q1: Can I inject Sustanon once every 2 weeks?
- Q2: Why do some doctors prescribe Sustanon every 3 weeks?
- Q3: Is Sustanon better than single-ester testosterone?
- Q4: Can I switch from Sustanon to another testosterone ester mid-cycle?
- Q5: Does injection site affect Sustanon half-life?
- Q6: Can I use Sustanon for TRT?
- The Bottom Line: Decanoate Dictates Everything
Understanding Steroid Half-Life (The Basics)
The essential pharmacokinetic concept.
What Half-Life Actually Means
The definition:
- Time required for half of the injected dose to be eliminated
- Pharmacokinetic measurement of drug clearance
- Applies to all drugs, not just steroids
- Fundamental concept
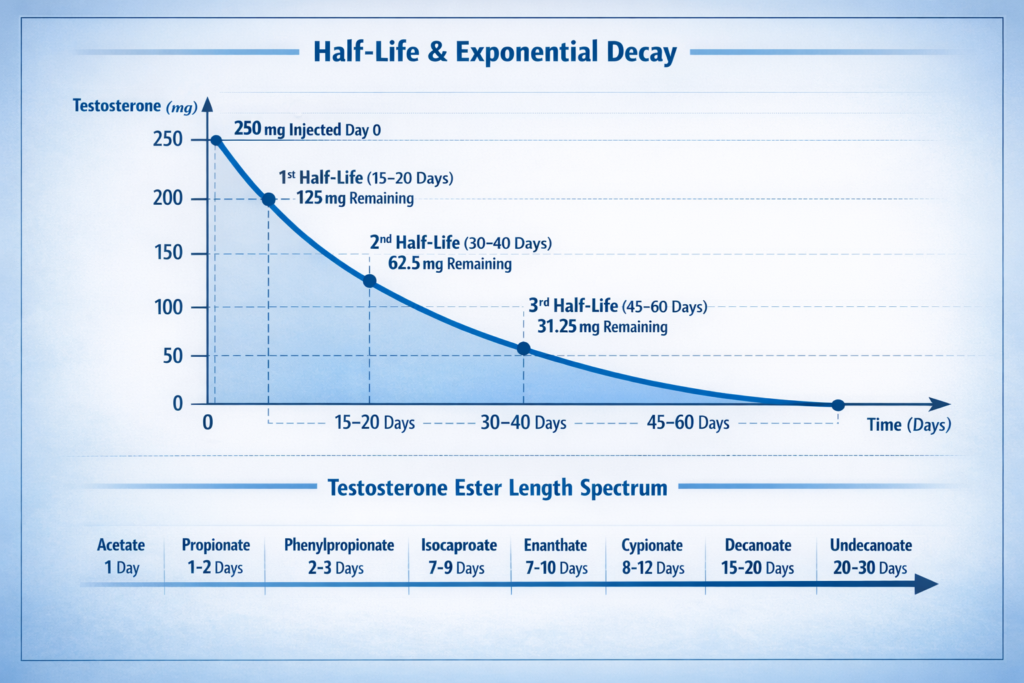
The example:
- Inject 250mg Sustanon
- After 15-20 days (one half-life): 125mg remains
- After another 15-20 days (two half-lives): 62.5mg remains
- After another 15-20 days (three half-lives): 31.25mg remains
- Exponential decay
The visualization:
- Not linear (doesn’t drop by same amount each day)
- Exponential curve (steep at first, then gradual)
- Never reaches absolute zero
- Decay pattern
Why this matters:
- Determines injection frequency
- Affects blood level stability
- Dictates PCT timing
- Influences side effect duration
- Practical implications
The Role of Esters
What esters are:
- Chemical chains attached to testosterone molecule
- Act as time-release mechanism
- Determine how fast testosterone is released
- Pharmacokinetic modifiers
How esters work:
After injection:
- Testosterone ester sits in muscle tissue
- Enzymes called “esterases” in the body
- Break the bond between testosterone and ester
- Enzymatic cleavage
The release process:
- Ester broken → Free testosterone released
- Enters bloodstream
- Ester length determines breakdown speed
- Controlled release
The relationship:
- Longer ester = Slower breakdown = Longer half-life
- Shorter ester = Faster breakdown = Shorter half-life
- Direct correlation
Common testosterone esters (shortest to longest):
- No ester (suspension): Hours (immediate release)
- Acetate: 1 day
- Propionate: 1-2 days
- Phenylpropionate: 2-3 days
- Isocaproate: 7-9 days
- Enanthate: 7-10 days
- Cypionate: 8-12 days
- Decanoate: 15-20 days
- Undecanoate: 20-30 days
- Half-life spectrum
Multiple Ester Formulations
The concept:
- Some products mix multiple esters
- Sustanon is the most famous example
- Omnadren is similar
- Blend approach
The marketing claim:
- “Fast-acting AND long-lasting”
- “Best of both worlds”
- “Stable levels”
- Theoretical benefits
The reality:
- Half-life ALWAYS determined by longest ester
- Shortest esters don’t significantly affect total duration
- More marketing than practical benefit
- Longest ester dominates
The rule:
- In multi-ester blends, ignore shorter esters for half-life calculations
- Only the longest ester matters
- Simplifying principle
Individual Variation in Half-Life
Why half-life ranges exist:
- Not exact science
- Individual variation occurs
- Population averages
Factors affecting half-life:
Genetics:
- Esterase enzyme activity varies
- Some people metabolize faster/slower
- Genetic variation
Metabolism:
- Faster metabolizers clear drugs quicker
- Slower metabolizers retain longer
- Metabolic rate
Age:
- Older individuals often metabolize slower
- Enzyme activity decreases with age
- Age-related changes
Body composition:
- Body fat percentage affects distribution
- Lipophilic (fat-soluble) drugs affected most
- Fat mass influence
Overall health:
- Liver and kidney function affect clearance
- Disease states alter pharmacokinetics
- Health status
The practical impact:
- Sustanon half-life: 15-20 days (not exact)
- Individual may be 14 days or 22 days
- Use average for planning
- Range, not precise number
Sustanon Composition and Half-Life
The four-ester breakdown.
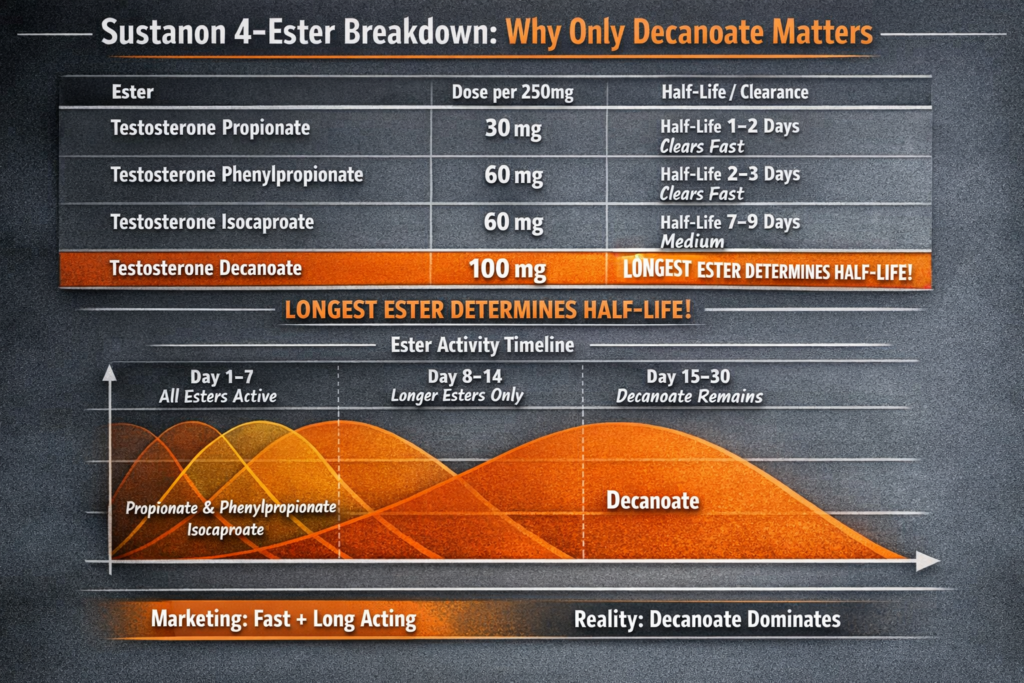
Sustanon’s Four Testosterone Esters
The formulation (per 1ml/250mg):
1. Testosterone Propionate: 30mg
- Half-life: 1-2 days
- Shortest ester in blend
- Fast-acting component
2. Testosterone Phenylpropionate: 60mg
- Half-life: 2-3 days
- Second shortest
- Medium-fast component
3. Testosterone Isocaproate: 60mg
- Half-life: 7-9 days
- Medium-length ester
- Medium component
4. Testosterone Decanoate: 100mg
- Half-life: 15-20 days
- Longest ester in blend
- Slow-release component
Total: 250mg testosterone (in various ester forms)
Why Only Decanoate Matters
The pharmacokinetic principle:
- Longest ester determines total duration
- Other esters clear while decanoate remains
- Longest ester dominates
The timeline visualization:
Day 1-2:
- Propionate peaks and begins clearing
- Phenylpropionate starting to peak
- Isocaproate and decanoate slowly releasing
- Multiple esters active
Day 3-7:
- Propionate mostly cleared
- Phenylpropionate clearing
- Isocaproate peaking
- Decanoate steadily releasing
- Shorter esters fading
Day 7-14:
- Propionate, phenylpropionate completely gone
- Isocaproate mostly cleared
- Decanoate still releasing (peak levels)
- Only longer esters remain
Day 15-30:
- Only decanoate remains
- Slowly declining
- Determines when levels drop significantly
- Decanoate alone
The conclusion:
- After first 2 weeks, only decanoate matters
- Half-life = decanoate half-life = 15-20 days
- Simple answer
The Marketing vs. Reality
The marketed benefit:
- “Combines fast-acting and long-lasting esters”
- “Provides immediate testosterone boost and sustained levels”
- “Best of both worlds”
- Sales pitch
The reality:
Immediate boost (propionate/phenylpropionate):
- Levels spike first few days
- Then drop as short esters clear
- Minimal practical benefit
- Temporary effect
Sustained levels (decanoate):
- Takes 4-6 weeks to reach steady state
- Short esters irrelevant after first week
- Same as using testosterone enanthate or cypionate alone
- No real advantage
The verdict:
- Sustanon works (it’s testosterone)
- But multi-ester blend doesn’t provide significant benefit over single long ester
- More expensive than single ester products
- Marketing over function
Why doctors use it:
- Historical precedent
- Pharmaceutical availability
- Patient familiarity
- Not because it’s superior
- Institutional inertia
Why users choose it:
- Brand recognition (Sustanon name well-known)
- Belief in marketing claims
- Availability in some regions
- Not because of pharmacokinetic advantages
- Perception over reality
Practical Implications: Injection Frequency
How often to inject Sustanon.
The Theoretical Range
Based on 15-20 day half-life:
- Could inject as infrequently as every 2-3 weeks
- One half-life = substantial hormone remaining
- Technically feasible
- Maximum spacing
The medical practice:
- Some doctors prescribe every 3 weeks (21 days)
- Particularly older protocols
- Based on half-life calculations
- Clinical approach
The problem with infrequent injections:
- Massive hormone fluctuations
- Peak levels first few days (too high)
- Trough levels before next injection (too low)
- Unstable blood levels
The Optimal Frequency: Once or Twice Weekly
Why more frequent is better:
Stable blood levels:
- Less fluctuation between peak and trough
- More consistent feeling day-to-day
- Reduced side effects
- Hormonal stability
Reduced side effects:
- Aromatization (estrogen conversion) related to testosterone spikes
- Mood swings related to hormone fluctuations
- Acne and oily skin worse with unstable levels
- Side effect management
Better results:
- Muscle growth optimized with stable anabolic environment
- Recovery consistent
- Performance predictable
- Outcome optimization
The protocols:
Once weekly injection:
- Standard for many users
- Example: 250mg every Monday
- Acceptable stability
- Convenient
- Common approach
Twice weekly injection:
- Better stability
- Example: 125mg Monday, 125mg Thursday
- Minimal fluctuation
- Optimal for most users
- Preferred approach
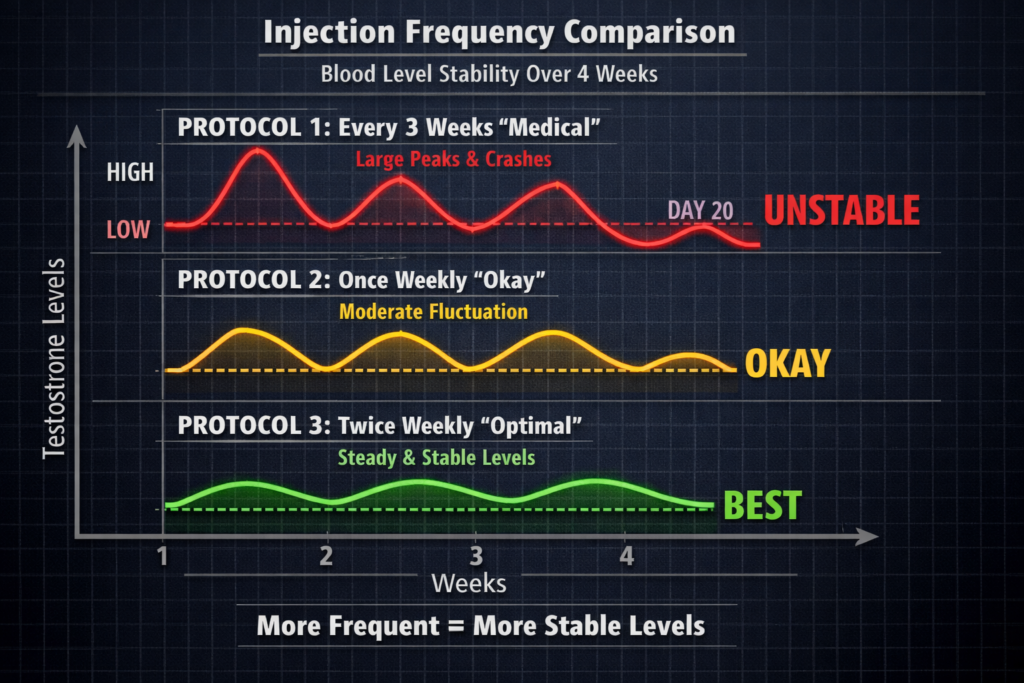
The comparison:
Every 3 weeks (medical protocol):
- Day 1: Very high levels
- Day 10: Moderate levels
- Day 20: Low levels (symptoms possible)
- Large fluctuation
Once weekly:
- Peak: 2-3 days post-injection
- Trough: Day 6-7 (before next injection)
- Moderate fluctuation
- Acceptable range
Twice weekly:
- Minimal peak-trough difference
- Stable levels throughout week
- Best approach
- Optimal stability
The Practical Recommendation
For TRT (therapeutic replacement):
- Twice weekly preferred (50-100mg each injection)
- Maintains stable physiological levels
- Minimizes side effects
- Medical use
For performance enhancement:
- Twice weekly standard (depends on total weekly dose)
- Example: 500mg/week = 250mg Monday, 250mg Thursday
- Stable supraphysiological levels
- Performance use
The flexibility:
- Decanoate’s long half-life means missing a day won’t crash levels
- Can adjust injection day by 1-2 days if needed
- Not as rigid as short esters (propionate requires precise timing)
- Forgiving schedule
PCT Timing After Sustanon
When to start post-cycle therapy.
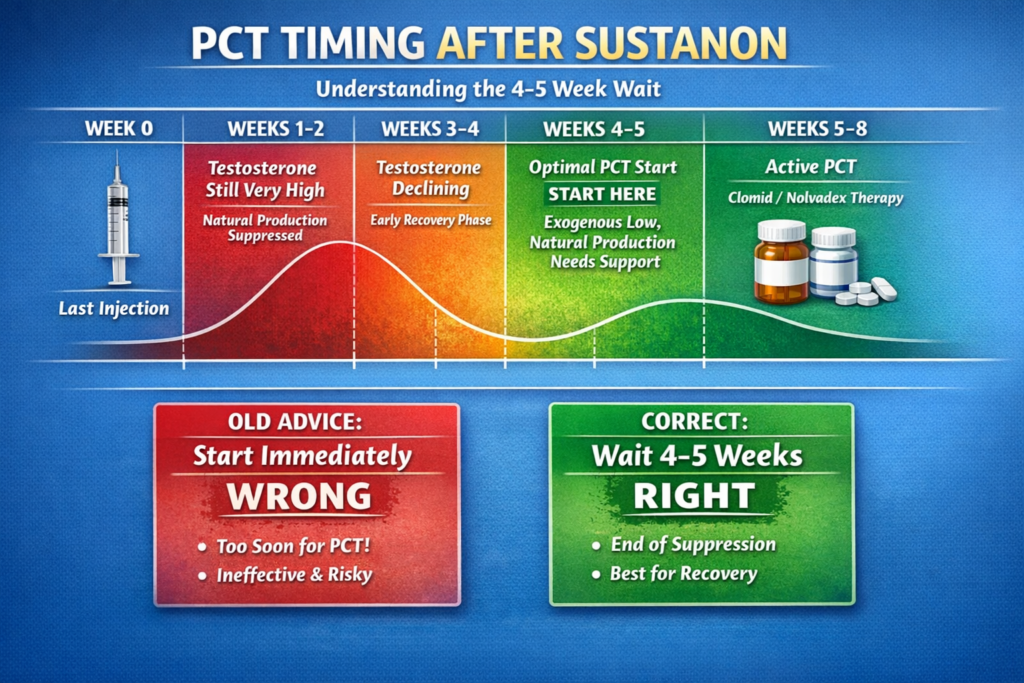
The Old Misconception
The outdated advice:
- “Start PCT immediately after last injection”
- Or: “Start PCT after one half-life”
- Wrong timing
Why this doesn’t work:
The problem:
- One half-life = 50% of dose still active
- Testosterone levels still suppressive
- Natural production still shut down
- PCT drugs (Clomid, Nolvadex) ineffective while exogenous testosterone elevated
- Premature initiation
The analogy:
- Like trying to restart a car while someone’s still holding the brake
- Natural production can’t recover while suppressed
- Futile effort
The Correct PCT Timing
The guideline:
- Wait 4-5 weeks after last Sustanon injection
- Then begin PCT
- Delayed start
The reasoning:
Week 1 post-injection:
- Testosterone levels still very high
- Natural production completely suppressed
- Too early for PCT
- Still suppressed
Week 2 post-injection:
- Testosterone declining but still elevated
- Natural production beginning to recover slightly
- Still too early
- Declining but suppressed
Week 3 post-injection:
- Testosterone significantly lower
- Natural production attempting recovery
- Getting closer
- Transition zone
Week 4-5 post-injection:
- Exogenous testosterone low enough
- Natural production needs support
- PCT drugs can now work effectively
- Optimal timing
The strategic approach:
- Start PCT while still some exogenous testosterone present
- Provides smooth transition (prevents crash)
- PCT drugs support natural production as exogenous clears
- Bridging strategy
Why Not Wait for Complete Clearance?
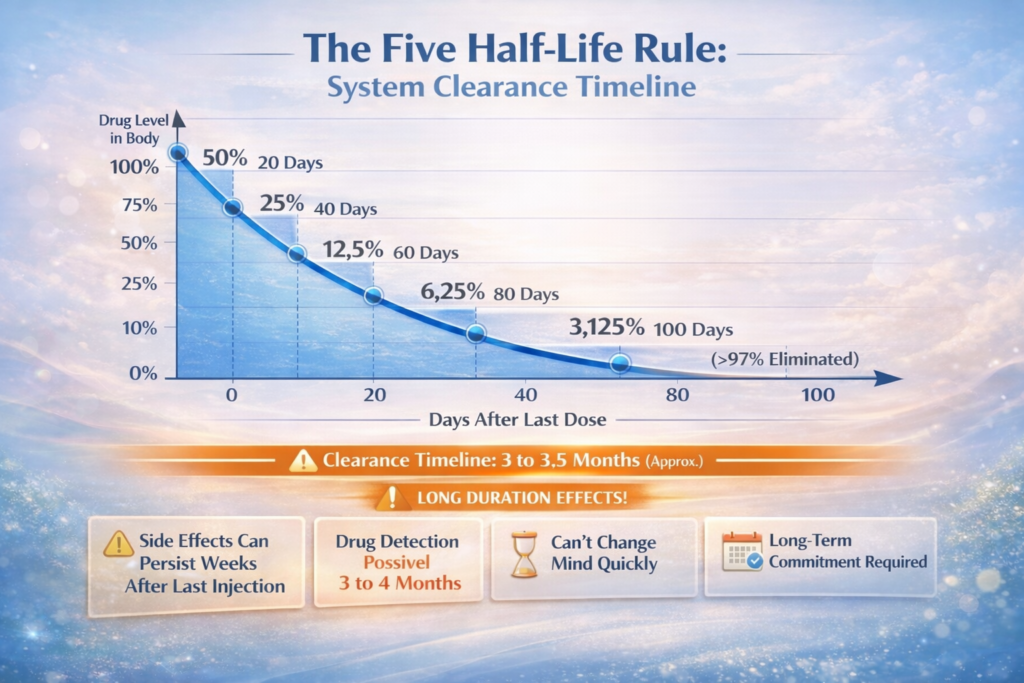
The 5 half-life rule:
- Complete elimination = 5 half-lives
- 15-20 days × 5 = 75-100 days (2.5-3.5 months)
- Very long wait
The problems with waiting that long:
Prolonged suppression:
- 3+ months with low testosterone
- Severe symptoms (fatigue, depression, libido loss)
- Muscle loss
- Miserable experience
Unnecessary suffering:
- By week 4-5, levels low enough for PCT to work
- No benefit to waiting additional 6-8 weeks
- Pointless delay
The balance:
- Start PCT when exogenous levels low enough
- But not so low that severe symptoms occur
- 4-5 weeks is sweet spot
- Optimal timing
Sample PCT Protocol After Sustanon
Week 0: Last Sustanon injection
Weeks 1-4: Waiting period
- No PCT drugs
- Testosterone declining
- Possible mild symptoms (manageable)
- Transition phase
Weeks 5-8: PCT (example protocol)
- Clomid: 50mg daily for 4 weeks
- Nolvadex: 20mg daily for 4 weeks
- Or other PCT protocol as designed
- Active recovery
Weeks 9+: Post-PCT
- Natural production recovering
- Monitor symptoms and consider bloodwork
- Assessment phase
Complete System Clearance
How long until Sustanon is completely gone.
The 5 Half-Life Rule
The pharmacokinetic principle:
- After 5 half-lives, >97% of drug eliminated
- Considered clinically insignificant levels
- Standard in pharmacology
- Clearance guideline
The calculation for Sustanon:
- One half-life: 15-20 days (use 20 for safety)
- Five half-lives: 20 × 5 = 100 days
- 3.5 months approximately
The timeline:
- Half-life 1 (20 days): 50% remains
- Half-life 2 (40 days): 25% remains
- Half-life 3 (60 days): 12.5% remains
- Half-life 4 (80 days): 6.25% remains
- Half-life 5 (100 days): 3.125% remains
- Exponential decline
Practical Implications
For side effects:
- If experiencing side effects from Sustanon
- They may persist for weeks after last injection
- Gradually diminishing as levels drop
- Complete resolution: 3+ months
- Side effect duration
The management:
- Can’t “speed up” clearance significantly
- Must manage symptoms during decline
- Estrogen-related sides (if occurring): AI may help temporarily
- Androgenic sides: Symptomatic treatment
- Symptom management
For detection (drug testing):
- Athletic drug tests can detect exogenous testosterone
- Detection window extends well beyond subjective effects
- Can be 3-4+ months for sensitive tests
- Anti-doping consideration
The important note:
- This article doesn’t focus on evading drug tests
- Mentioned for completeness only
- Cheating in sports = ethical violation
- Not our purpose
For health recovery:
- Cardiovascular parameters begin improving as levels drop
- Lipid profile starts normalizing
- But takes time (months)
- Regular monitoring important
- Recovery timeline
Why This Matters Before Using
The informed decision:
- Before first injection, understand commitment
- Long ester = prolonged effects (good and bad)
- Can’t change mind and have it gone next week
- Long-term commitment
The comparison:
Testosterone propionate (short ester):
- Half-life: 1-2 days
- Complete clearance: 5-10 days
- Side effects resolve quickly
- Easy to manage
- Fast in, fast out
Sustanon (long ester dominant):
- Half-life: 15-20 days
- Complete clearance: 75-100 days
- Side effects persist
- Difficult to manage if problematic
- Slow in, slow out
The consideration:
- First-time users might prefer shorter esters (easier to manage)
- Experienced users comfortable with long esters
- Experience-dependent choice
Sustanon vs. Other Testosterone Esters
Comparison context.
Sustanon vs. Testosterone Enanthate
Testosterone Enanthate:
- Single ester
- Half-life: 7-10 days
- Standard long-acting testosterone
- Single-ester alternative
The comparison:
Half-life:
- Sustanon: 15-20 days (decanoate)
- Enanthate: 7-10 days
- Sustanon slightly longer
- Sustanon longer
Injection frequency:
- Both can be injected 1-2x weekly for stable levels
- Enanthate slightly more forgiving (shorter half-life = faster adjustment)
- Minimal practical difference
- Similar protocols
PCT timing:
- Sustanon: Wait 4-5 weeks
- Enanthate: Wait 2-3 weeks
- Sustanon requires longer wait
- Sustanon longer wait
Cost:
- Sustanon often more expensive (multi-ester manufacturing)
- Enanthate usually cheaper
- Same active hormone (testosterone)
- Enanthate more economical
The verdict:
- No significant advantage to Sustanon over enanthate
- Enanthate simpler and cheaper
- Both work effectively
- Enanthate preferred by many
Sustanon vs. Testosterone Cypionate
Testosterone Cypionate:
- Single ester
- Half-life: 8-12 days
- Popular in US
- US standard
The comparison:
- Very similar to enanthate comparison
- Cypionate half-life between enanthate and Sustanon
- Practically interchangeable with enanthate
- All three (Sustanon, enanthate, cypionate) are long-acting
- Minimal differences
Sustanon vs. Testosterone Propionate
Testosterone Propionate:
- Single ester
- Half-life: 1-2 days
- Short-acting testosterone
- Short-ester alternative
The comparison:
Injection frequency:
- Propionate: Every day or every other day (strict schedule)
- Sustanon: 1-2x weekly
- Sustanon much more convenient
- Sustanon advantage
Blood level stability:
- Propionate: Very stable (due to frequent injections)
- Sustanon: Moderate fluctuation (even with 2x weekly)
- Propionate technically superior for stability if injecting daily
- Propionate advantage (if disciplined)
PCT timing:
- Propionate: 3-5 days after last injection
- Sustanon: 4-5 weeks after last injection
- Propionate much faster
- Propionate advantage
Side effect management:
- Propionate: Adjust quickly (stops in days)
- Sustanon: Persists for weeks
- Propionate easier to manage
- Propionate advantage
Convenience:
- Propionate: Daily injections (burden)
- Sustanon: Weekly injections (easy)
- Sustanon wins on convenience
- Sustanon advantage
The verdict:
- Propionate for those wanting control and willing to inject daily
- Sustanon for convenience
- Different use cases
- Context-dependent
Common Questions
Addressing specific concerns.
Q1: Can I inject Sustanon once every 2 weeks?
The answer:
- Technically possible (based on half-life)
- But not optimal
- Technically yes, practically no
The problems:
- Large fluctuations in testosterone levels
- First week: Very high (potential side effects)
- Second week: Declining (potential symptoms)
- Unstable levels
The better approach:
- Split into 2 injections weekly
- More stable levels
- Better results and fewer sides
- Prefer frequent dosing
Q2: Why do some doctors prescribe Sustanon every 3 weeks?
The reasons:
Outdated protocols:
- Based on half-life alone
- Not considering patient experience
- Old pharmaceutical recommendations
- Legacy practice
Cost considerations:
- Fewer injections = fewer clinic visits
- Less nursing time
- Administrative convenience
- Economic factors
Patient convenience (perceived):
- Some patients prefer infrequent injections
- Willing to tolerate fluctuations
- Individual preference
The reality:
- Not optimal for stable levels
- Modern TRT protocols favor more frequent dosing
- Patients often feel better with weekly or twice-weekly
- Improved protocols available
Q3: Is Sustanon better than single-ester testosterone?
The answer:
- Not significantly better
- Marketing suggests advantages
- Practical experience shows minimal difference
- Marketing over reality
The claimed advantages:
- “Fast-acting and long-lasting”
- “Best of both worlds”
- Sales pitch
The reality:
- All long-acting testosterones provide sustained levels
- Short esters in Sustanon clear quickly (irrelevant long-term)
- No proven superiority in studies
- Functionally equivalent
The disadvantages:
- More expensive
- Complex formulation (no benefit)
- Longer PCT wait time (vs. enanthate/cypionate)
- Potential downsides
Q4: Can I switch from Sustanon to another testosterone ester mid-cycle?
The answer:
- Yes, you can switch
- Switchable
The process:
Switching to longer ester (Sustanon to undecanoate):
- Overlap not necessary (both long-acting)
- Stop Sustanon, start undecanoate next injection day
- Direct switch
Switching to shorter ester (Sustanon to propionate):
- Can switch immediately
- Propionate injections begin
- Sustanon decanoate continues declining in background
- Levels remain elevated
- Overlapping effect
Switching to similar ester (Sustanon to enanthate/cypionate):
- Direct switch on next injection day
- Minimal change in blood levels
- Seamless transition
The PCT consideration:
- PCT timing based on last injection of LONGEST ester used
- If switched from Sustanon to enanthate, wait based on enanthate
- If switched from enanthate to Sustanon, wait based on Sustanon (decanoate)
- Last injection determines PCT timing
Q5: Does injection site affect Sustanon half-life?
The answer:
- Minor effect, clinically insignificant
- Minimal impact
The theory:
- Different injection sites have different blood flow
- Higher blood flow = slightly faster absorption
- Theoretical variation
The reality:
- Difference is small (maybe 10-15% variation)
- All intramuscular sites provide depot effect
- Half-life remains 15-20 days regardless
- Insignificant practical difference
The sites:
- Glutes, quads, delts all acceptable
- Rotate sites for comfort
- Don’t overthink absorption differences
- Any IM site works
Q6: Can I use Sustanon for TRT?
The answer:
- Yes, commonly used for TRT
- Particularly outside US
- TRT-appropriate
The protocol:
- Typical TRT dose: 100-200mg Sustanon per week
- Injected once or twice weekly
- Maintains physiological testosterone levels
- Standard TRT approach
The monitoring:
- Regular bloodwork (testosterone, estradiol, hematocrit, lipids)
- Adjust dose based on levels and symptoms
- Target mid-normal testosterone range
- Medical supervision
The alternatives:
- Testosterone enanthate or cypionate work equally well
- Often cheaper and simpler
- US more commonly uses enanthate/cypionate
- Europe/Asia more commonly uses Sustanon
- Regional preferences
The Bottom Line: Decanoate Dictates Everything
After explaining everything:
The truth about Sustanon half-life:
✅ Sustanon half-life is 15-20 days (determined by testosterone decanoate)
✅ Only the longest ester matters for half-life calculations (other three esters irrelevant)
✅ Inject 1-2x weekly for stable levels (not every 2-3 weeks despite long half-life)
✅ Wait 4-5 weeks after last injection to start PCT (not immediately or after one half-life)
✅ Complete system clearance takes 75-100 days (3+ months using 5 half-life rule)
Key takeaways:
Sustanon composition:
- 30mg testosterone propionate (half-life 1-2 days)
- 60mg testosterone phenylpropionate (half-life 2-3 days)
- 60mg testosterone isocaproate (half-life 7-9 days)
- 100mg testosterone decanoate (half-life 15-20 days)
- Total: 250mg testosterone per ml
- Four ester blend
Half-life determination:
- Longest ester (decanoate) determines half-life
- Other esters clear within 1-2 weeks
- Decanoate remains for months
- Half-life = 15-20 days
- Decanoate dominates
The math:
- 250mg injected
- After 15-20 days: 125mg remains
- After 30-40 days: 62.5mg remains
- After 45-60 days: 31.25mg remains
- Exponential decay
Optimal injection frequency:
- Once weekly: Acceptable (example: 250mg every Monday)
- Twice weekly: Preferred (example: 125mg Monday, 125mg Thursday)
- Every 2-3 weeks: Possible but poor (large fluctuations)
- More frequent = more stable
Why frequent matters:
- Stable blood testosterone levels
- Reduced side effects (aromatization, mood, acne)
- Better results (consistent anabolic environment)
- Stability benefits
PCT timing:
- Old advice: Start immediately or after 1 half-life (WRONG)
- Correct timing: 4-5 weeks after last injection
- Reason: Levels must drop enough for PCT to work, but not so low that severe symptoms occur
- Strategic delay
PCT timeline:
- Week 0: Last injection
- Weeks 1-4: Waiting (testosterone declining)
- Weeks 5-8: Active PCT (Clomid/Nolvadex)
- Weeks 9+: Recovery monitoring
- 4-5 week wait essential
Complete clearance:
- 5 half-lives = >97% eliminated
- 15-20 days × 5 = 75-100 days
- Approximately 3-3.5 months
- Long clearance time
Practical implications:
- Side effects persist for weeks after last injection
- Drug detection possible for 3-4 months
- Can’t “change mind” quickly
- Long-term commitment
Sustanon vs. other esters:
- vs. Enanthate/Cypionate: Longer half-life, longer PCT wait, more expensive, no real advantage
- vs. Propionate: More convenient (less frequent injections), but less control, longer clearance
- Trade-offs exist
Individual variation:
- Half-life ranges (15-20 days, not exact)
- Genetics, metabolism, age, body composition affect clearance
- Use average for planning
- Personal variation exists
For TRT use:
- 100-200mg weekly (split into 1-2 injections)
- Maintains physiological levels
- Medical supervision essential
- Regular bloodwork required
- Therapeutic application
SUSTANON HALF-LIFE = 15-20 DAYS (DECANOATE ESTER). INJECT 1-2X WEEKLY FOR STABILITY. START PCT 4-5 WEEKS POST-INJECTION. COMPLETE CLEARANCE: 3+ MONTHS. UNDERSTAND BEFORE FIRST INJECTION.
This article is informational only. We do not condone or recommend steroid use. If considering any hormone therapy, work with qualified medical professionals and understand the serious health risks involved.
REFERENCES
SECTION 1 — Sustanon Composition and Testosterone Ester Half-Lives
[1] Pastuszak AW et al. — Andrology (Wiley), 2022 Pharmacokinetics of testosterone therapies in relation to diurnal variation of serum testosterone levels as men age — confirms Sustanon 250 composition (30mg propionate, 60mg phenylpropionate, 60mg isocaproate, 100mg decanoate); in silico simulations show multi-ester blends produce wider testosterone fluctuations than single-ester formulations https://pmc.ncbi.nlm.nih.gov/articles/PMC9293229/
[2] Handelsman DJ et al. — Clinical Endocrinology (Nieschlag Chapter Reference), 2002 Pharmacokinetics of testosterone — testosterone decanoate elimination half-life 20.9 days in tea seed oil, 33.9 days in castor oil; testosterone propionate 0.8 days, enanthate 4.5 days; longest ester determines duration of depot release https://en.wikipedia.org/wiki/Pharmacokinetics_of_testosterone
[3] Muram D et al. — Journal of Clinical Endocrinology and Metabolism, 2002 Investigation of a novel preparation of testosterone decanoate in men: pharmacokinetics and spermatogenic suppression — 20 healthy men administered 400mg TD intramuscularly every 4 weeks; trough testosterone rose with repeated administration, demonstrating decanoate’s long-acting release profile https://pubmed.ncbi.nlm.nih.gov/12443967/
SECTION 2 — Injection Frequency and Blood Level Stability
[4] Spinner ML et al. — Translational Andrology and Urology (PMC), 2016 Pharmacology of testosterone replacement therapy preparations — 200mg testosterone cypionate every 2 weeks caused a threefold rise in serum testosterone peaking at days 4-5 (1,112 ng/dL), then declining to ~400 ng/dL by day 14; “these large fluctuations illustrate the less than ideal kinetics” of infrequent dosing https://pmc.ncbi.nlm.nih.gov/articles/PMC5182226/
[5] Snyder PJ, Lawrence DA — Journal of Clinical Endocrinology and Metabolism, 1980 (referenced in Pastuszak 2022) Treatment of male hypogonadism with testosterone enanthate — evaluated 100mg weekly, 200mg biweekly, 300mg every 3 weeks, 400mg every 4 weeks; 100mg/week and 200mg/2 weeks best maintained testosterone in normal range; weekly dosing produces more stable levels https://pmc.ncbi.nlm.nih.gov/articles/PMC9293229/
[6] Nair AS et al. — Journal of the Endocrine Society (Oxford Academic), 2017 Serum testosterone concentrations remain stable between injections in patients receiving subcutaneous testosterone — 11 patients on weekly testosterone cypionate; total and free testosterone remained stable and within normal male range throughout the entire dosing interval https://pmc.ncbi.nlm.nih.gov/articles/PMC5686655/
SECTION 3 — PCT Timing: SERMs and HPG Axis Recovery
[7] Wenker EP et al. — PMC / Translational Andrology and Urology, 2015 (referenced in Rahnema 2014) Recovery of spermatogenesis following testosterone replacement therapy or anabolic-androgenic steroid use — SERMs (clomiphene/tamoxifen) block estrogen’s negative feedback on the hypothalamus and pituitary, restoring LH, FSH, and endogenous testosterone production; PCT drugs ineffective while exogenous testosterone levels remain suppressive https://pmc.ncbi.nlm.nih.gov/articles/PMC4854084/
[8] Hohl A et al. — Clomiphene Citrate Treatment as Alternative for Male Hypogonadism — MDPI Pharmaceuticals, 2024 Clomiphene citrate treatment as an alternative therapeutic approach for male hypogonadism — clomiphene resulted in significant increases in total testosterone, LH, and FSH; SERMs restore endogenous production by blocking estrogen’s inhibitory feedback on the HPG axis; mechanism confirms why PCT must wait for exogenous testosterone to drop https://pmc.ncbi.nlm.nih.gov/articles/PMC11435126/
SECTION 4 — Complete System Clearance (5 Half-Life Rule)
[9] Nieschlag E — Clinical Endocrinology (Wiley), 2006 Testosterone treatment comes of age: new options for hypogonadal men — esterification of testosterone at position 17 with long aliphatic side chains (enanthate, cypionate, decanoate) creates injectable depot preparations; traditional 2-3 week injectable esters cause supraphysiological peaks then subtherapeutic troughs; long ester clearance follows exponential pharmacokinetic decay https://onlinelibrary.wiley.com/doi/10.1111/j.1365-2265.2006.02618.x




Leave a Reply
You must be logged in to post a comment.