Low energy? No motivation? Losing muscle and gaining fat? Your testosterone is probably crashed.
You used to wake up ready to conquer the world. Now you hit snooze five times.
You’re training hard but looking soft. Your sex drive is nonexistent. You feel like a shell of your former self.
You’ve heard about “low T” but think it only affects old men:
- You’re only 30-something
- You eat relatively healthy
- You exercise regularly
- Should be fine, right?
Wrong. Testosterone levels in men have dropped 20-30% in the last 30 years. Average 30-year-old today has testosterone of a 50-year-old from the 1980s. This isn’t aging. This is environmental.
Here’s what’s actually happening: Modern lifestyle systematically destroys testosterone. Poor sleep, chronic stress, obesity, processed foods, sedentary behavior, environmental toxins, and overtraining all crash your levels. Most men are walking around with testosterone 200-400 ng/dL (technically “normal” but functionally low). Optimal is 700-1000+ ng/dL. The difference between 300 and 800 is night and day: energy, strength, muscle mass, fat loss, mood, motivation, and performance all dramatically different.
In this comprehensive guide, I’ll explain why testosterone matters more than you think (affects everything), reveal the 9 evidence-based strategies to optimize it naturally (no TRT needed for most people), show you the lifestyle factors systematically destroying your testosterone (fix these first), provide the complete supplement protocol that actually works (most supplements are scams), and explain when medical intervention becomes necessary (and how to work with doctors).
Whether you’re 25 or 55, optimizing testosterone transforms your life.
Let’s restore your testosterone to optimal levels naturally.
TABLE OF CONTENTS
- Strategy 1: Lose Excess Body Fat (Most Powerful)
- Strategy 2: Optimize Sleep (Non-Negotiable)
- Strategy 3: Resistance Training (Progressive Overload)
- Strategy 4: Optimize Vitamin D Levels
- Strategy 5: Manage Stress Effectively
- Strategy 6: Eat Adequate Healthy Fats
- Strategy 7: Optimize Zinc and Magnesium Intake
- Strategy 8: Practice Time-Restricted Eating
- Strategy 9: Cold Exposure (Testicular Cooling)
- The Bottom Line: Optimize Testosterone Naturally
What Is Testosterone and Why Does It Matter?
Understanding the master male hormone.
Testosterone: More Than Just Sex Hormone
What it is:
- Primary male sex hormone (androgen)
- Produced in testes (95%) and adrenal glands (5%)
- Regulates countless physiological processes
- Declines with age but should remain adequate
- Master male hormone
What it does:
Physical effects:
- Builds muscle mass and strength
- Reduces body fat (especially visceral)
- Increases bone density
- Deepens voice (puberty)
- Promotes facial and body hair
- Masculinizing hormone
Metabolic effects:
- Increases metabolic rate
- Improves insulin sensitivity
- Enhances fat oxidation
- Regulates glucose metabolism
- Metabolic optimizer
Cognitive/Psychological effects:
- Improves mood and motivation
- Reduces depression and anxiety
- Enhances confidence and assertiveness
- Improves spatial reasoning
- Supports memory
- Mental performance
Sexual effects:
- Drives libido and sexual function
- Supports erectile function
- Maintains reproductive health
- Sexual health
Why it matters for physique:
- High testosterone = easy muscle gain, easy fat loss
- Low testosterone = muscle loss, fat gain (especially belly)
- Determines body composition response to training
- Physique foundation
Normal vs. Optimal Testosterone Levels
The ranges:
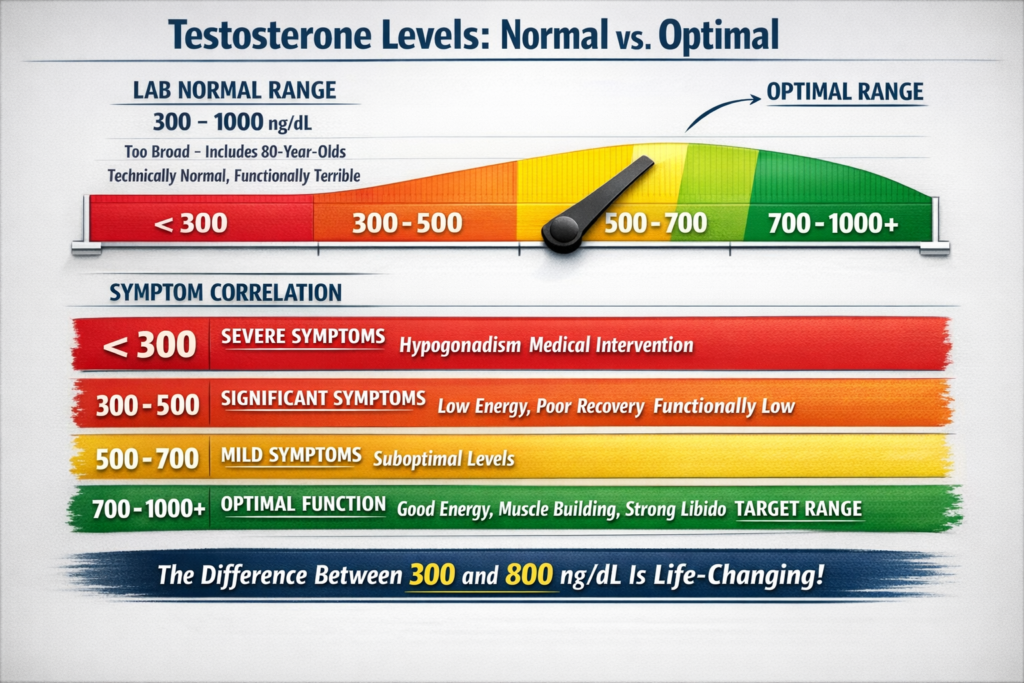
Lab “normal” range:
- 300-1000 ng/dL (total testosterone)
- If you’re 301, doctor says “you’re normal”
- Technically normal, functionally terrible
The problem with “normal”:
- Range includes 80-year-old men
- Average has dropped dramatically
- Many symptomatic men test “normal”
- Normal ≠ optimal
Optimal ranges (for men under 50):
- Total testosterone: 700-1000+ ng/dL
- Free testosterone: 15-25+ pg/mL
- Bioavailable testosterone: 150-300+ ng/dL
- Where you want to be
Age-related decline:
- Begins around age 30
- Drops ~1-2% per year
- By age 70, often 50% lower
- But lifestyle factors accelerate this dramatically
- Not inevitable
Symptom correlation:
Below 300 ng/dL:
- Severe symptoms
- Medical intervention often needed
- Classified as hypogonadism
- Clinical low testosterone
300-500 ng/dL:
- Significant symptoms
- Low energy, poor recovery
- Difficult muscle building
- Fat gain, especially midsection
- Low libido
- Functionally low
500-700 ng/dL:
- Mild symptoms
- Not optimal but manageable
- Room for improvement
- Suboptimal
700-1000+ ng/dL:
- Optimal function
- Good energy and recovery
- Muscle building easy
- Leanness maintained
- Strong libido
- Target range
The difference:
- Man at 350 ng/dL vs. 850 ng/dL
- Completely different physique
- Completely different energy
- Completely different quality of life
- Massive impact
Signs of Low Testosterone
Physical symptoms:
- Decreased muscle mass (despite training)
- Increased body fat (especially belly)
- Reduced strength and endurance
- Chronic fatigue (not improved by sleep)
- Gynecomastia (breast tissue development)
- Body composition changes
Sexual symptoms:
- Low libido (reduced sexual desire)
- Erectile dysfunction
- Reduced morning erections
- Decreased fertility
- Sexual health decline
Cognitive/Emotional symptoms:
- Depression and anxiety
- Irritability and mood swings
- Reduced motivation and drive
- Brain fog and poor concentration
- Lack of confidence
- Mental health effects
Other symptoms:
- Hot flashes and sweating
- Sleep disturbances
- Reduced bone density
- Decreased body hair growth
- Systemic effects
The pattern:
- Multiple symptoms together
- Progressive worsening
- Affects quality of life significantly
- Cluster of issues
What’s Destroying Your Testosterone
Modern lifestyle factors systematically lowering testosterone.
Factor 1: Obesity and Body Fat
The mechanism:
- Fat tissue contains aromatase enzyme
- Aromatase converts testosterone to estrogen
- More fat = more aromatase = more conversion
- Fat literally destroys testosterone
The vicious cycle:
- Low testosterone → easier fat gain
- More fat → lower testosterone
- Cycle perpetuates
- Self-worsening
Visceral fat most problematic:
- Belly fat highest in aromatase
- Inflammatory cytokines from visceral fat
- Directly suppress testosterone production
- Abdominal fat worst
The research:
- Every 4-point increase in BMI
- Associated with ~75 ng/dL decrease in testosterone
- Significant effect
- Obesity major factor
The solution:
- Lose body fat (especially visceral)
- Get under 15% body fat (men)
- Testosterone will rise significantly
- Fat loss = testosterone increase
Factor 2: Poor Sleep Quality
The mechanism:
- Testosterone produced during sleep
- Primarily during REM sleep
- Poor sleep = reduced production
- Sleep is when testosterone made
The research:
- 5 hours sleep vs. 8 hours sleep
- 15% decrease in testosterone
- One week of sleep restriction
- Rapid decline
Chronic sleep deprivation:
- Sustained low testosterone
- Elevated cortisol (further suppresses testosterone)
- Multiple hormone disruptions
- Compounding problem
Sleep apnea:
- Disrupts sleep architecture
- Reduces REM sleep
- Significantly lowers testosterone
- Common but undiagnosed
- Hidden factor
The solution:
- 7-9 hours quality sleep nightly
- Consistent schedule
- Address sleep apnea if present
- Non-negotiable
Factor 3: Chronic Stress and High Cortisol
The mechanism:
- Stress elevates cortisol
- Cortisol and testosterone inversely related
- High cortisol suppresses testosterone production
- Stress response inhibits sex hormones
Why this happens:
- Evolutionary perspective
- Stress = danger = not time to reproduce
- Body prioritizes survival over reproduction
- Sex hormone production suppressed
- Biological tradeoff
Modern chronic stress:
- Work stress constant
- Financial worries
- Relationship issues
- Information overload
- Cortisol never drops
- Sustained suppression
Overtraining:
- Exercise is stress
- Excessive training elevates cortisol chronically
- Suppresses testosterone
- Common in dedicated lifters
- Too much of good thing
The solution:
- Manage stress actively
- Adequate recovery between workouts
- Meditation and breathing practices
- Address life stressors
- Stress management essential
Factor 4: Sedentary Lifestyle
The mechanism:
- Physical activity stimulates testosterone production
- Inactivity allows decline
- Muscle loss accelerates testosterone decline
- Use it or lose it
The research:
- Sedentary men have lower testosterone
- Resistance training acutely elevates testosterone
- Regular exercise maintains healthy levels
- Activity crucial
But overtraining worse:
- Marathon runners often have low testosterone
- Excessive cardio suppresses testosterone
- Need balance
- Goldilocks zone
The solution:
- Regular resistance training (3-4x weekly)
- Moderate cardio (not excessive)
- Daily movement (walking)
- Active lifestyle
Factor 5: Poor Diet Quality
The mechanisms:
Insufficient healthy fats:
- Testosterone synthesized from cholesterol
- Low fat diets lower testosterone
- Need adequate dietary fat
- Fat is precursor
Insufficient calories:
- Chronic calorie restriction suppresses testosterone
- Body perceives famine
- Reproduction deprioritized
- Undereating kills testosterone
High sugar/processed foods:
- Blood sugar spikes increase insulin
- High insulin suppresses testosterone
- Inflammation from processed foods
- Poor diet quality
Micronutrient deficiencies:
- Zinc, magnesium, vitamin D critical
- Most people deficient
- Direct role in testosterone production
- Nutrient insufficiency
The solution:
- Adequate calories (especially when training)
- 25-30% calories from healthy fats
- Whole food diet
- Address micronutrient deficiencies
- Nutrition optimization
Factor 6: Environmental Toxins
The xenoestrogens:
- Chemicals that mimic estrogen
- Bind to estrogen receptors
- Disrupt hormonal balance
- Endocrine disruptors
Common sources:
Plastics:
- BPA and phthalates
- Leach into food and water
- Heating plastic worse
- Everywhere
Pesticides:
- Herbicides and insecticides
- Especially on conventional produce
- Accumulate in body
- Food supply
Personal care products:
- Parabens in lotions, shampoos
- Triclosan in soaps
- Absorb through skin
- Daily exposure
Household products:
- Cleaning chemicals
- Air fresheners
- Non-stick cookware
- Home environment
The effect:
- Lower testosterone
- Higher estrogen
- Hormonal imbalance
- Cumulative exposure
The solution:
- Minimize plastic use (glass/steel containers)
- Choose organic produce (especially “Dirty Dozen”)
- Natural personal care products
- Reduce chemical exposure
- Environmental cleanup
Factor 7: Excess Alcohol
The mechanism:
- Alcohol impairs testosterone synthesis in testes
- Increases aromatase activity (testosterone → estrogen)
- Damages Leydig cells (testosterone-producing cells)
- Direct toxicity
The research:
- Even moderate drinking lowers testosterone
- Binge drinking acutely crashes testosterone for days
- Chronic heavy drinking causes sustained suppression
- Dose-dependent effect
The recommendation:
- Limit to 2-3 drinks per week maximum
- No binge drinking
- Alcohol-free days majority of week
- Moderation or abstinence
Factor 8: Certain Medications
Common culprits:
Opioid pain medications:
- Directly suppress testosterone production
- Major cause of low T
- Significant effect
Statins (cholesterol medications):
- Reduce cholesterol (testosterone precursor)
- May lower testosterone
- Indirect effect
Antidepressants (SSRIs):
- Can lower testosterone
- Affect sexual function
- Potential side effect
Corticosteroids:
- Suppress testosterone production
- If used chronically
- Hormonal suppression
The approach:
- Don’t stop medications without doctor
- Discuss alternatives if possible
- Monitor testosterone if on these medications
- Medical supervision

9 Evidence-Based Ways to Increase Testosterone Naturally
The complete optimization protocol.
Strategy 1: Lose Excess Body Fat (Most Powerful)
Why it works:
- Reduces aromatase activity (less testosterone → estrogen conversion)
- Decreases inflammatory cytokines
- Improves insulin sensitivity (insulin/testosterone relationship)
- Multiple mechanisms
The research:
- Obese men losing 10% body weight
- Average testosterone increase: 100-150 ng/dL
- Some see increases of 200-300 ng/dL
- Dramatic effect
The protocol:
Target body fat:
- Under 15% for men (optimal)
- Under 20% minimum
- Lower body fat = higher testosterone
- Leanness matters
How to lose fat:
- Moderate calorie deficit (300-500 calories)
- High protein (1g per pound body weight)
- Resistance training (preserve muscle)
- Sufficient fat intake (25-30% of calories)
- Sustainable approach
Important:
- Don’t crash diet (too aggressive deficit lowers testosterone)
- Don’t overdo cardio (excess stress)
- Maintain adequate calories
- Moderate approach
Timeline:
- Lose 1-2 pounds per week
- For every 10 pounds lost, expect 50-100 ng/dL increase
- Progressive improvement
- Steady progress
Strategy 2: Optimize Sleep (Non-Negotiable)
Why it’s critical:
- Testosterone produced during sleep
- 60% of daily testosterone during sleep
- Sleep deprivation immediately lowers levels
- Production window
The research:
- Men sleeping 4 hours have testosterone of men 10-15 years older
- 7-9 hours optimal
- Consistent schedule crucial
- Sleep duration matters
The protocol:
Sleep duration:
- 7-9 hours nightly (minimum 7)
- Consistent schedule (same bedtime/wake time)
- Consistency critical
Sleep quality:
- Dark room (blackout curtains)
- Cool temperature (65-68°F)
- No screens 1 hour before bed
- No caffeine after 2 PM
- Sleep hygiene
Sleep apnea:
- Get tested if suspected (snoring, morning fatigue, neck >17 inches)
- Apnea drastically lowers testosterone
- Treatment restores testosterone
- Common hidden cause
Supplements if needed:
- Magnesium glycinate (400mg before bed)
- Melatonin (0.5-3mg)
- L-theanine (200mg)
- Sleep support
Expected improvement:
- Fixing sleep: 50-150 ng/dL increase
- One of most powerful interventions
- Massive impact
Strategy 3: Resistance Training (Progressive Overload)
Why it works:
- Acute testosterone spike during/after training
- Chronic elevation with regular training
- Builds muscle (muscle supports testosterone)
- Direct stimulus
The research:
- Compound movements increase testosterone acutely
- Heavy weights (70-85% 1RM) most effective
- Volume and intensity both matter
- Regular training maintains healthy levels
- Well-documented
The protocol:
Exercise selection:
- Compound movements (multi-joint)
- Squats, deadlifts, bench press, rows, overhead press
- Use large muscle groups
- Big movements
Training parameters:
- 3-4 sessions per week
- 6-12 reps per set
- 70-85% of 1RM
- 3-4 exercises per session
- 3-4 sets per exercise
- Moderate volume, high intensity
Progressive overload:
- Increase weight over time
- Add reps
- Add sets
- Progression is key
- Continuous challenge
What NOT to do:
- Excessive training (overtraining lowers testosterone)
- Hours of cardio daily (endurance athletes often have low testosterone)
- No recovery days
- Avoid overtraining
Expected improvement:
- Acute: 15-25% increase during/after training
- Chronic: 20-40% increase with consistent training
- Powerful intervention
Strategy 4: Optimize Vitamin D Levels
Why it matters:
- Vitamin D is steroid hormone precursor
- Receptors in testes
- Directly involved in testosterone production
- Most people deficient
- Critical nutrient
The research:
- Men with vitamin D >30 ng/mL have higher testosterone
- Supplementation in deficient men increases testosterone
- Average increase: 20-30%
- Significant effect
The protocol:
Testing:
- Get 25-hydroxyvitamin D blood test
- Optimal: 40-60 ng/mL
- Most people <30 ng/mL (deficient)
- Test, don’t guess
Supplementation:
- If deficient: 4000-5000 IU daily
- With vitamin K2 (100-200mcg) for proper calcium regulation
- Take with fat-containing meal (fat-soluble)
- Daily supplementation
Retest:
- After 3 months
- Adjust dose to reach optimal range
- Maintain year-round
- Monitor levels
Expected improvement:
- If deficient: 100-200 ng/dL increase
- One of easiest interventions
- High return on investment
Strategy 5: Manage Stress Effectively
Why it’s critical:
- Cortisol directly suppresses testosterone
- Chronic stress major testosterone killer
- Must be addressed
- Stress-testosterone inverse relationship
The protocol:
Daily stress management:
Meditation:
- 10-20 minutes daily
- Reduces cortisol significantly
- Evidence-based
- Apps: Headspace, Calm
- Proven effective
Deep breathing:
- Box breathing (4-4-4-4)
- 4-7-8 breathing
- 5-10 minutes, 2-3x daily
- Activates parasympathetic nervous system
- Immediate stress relief
Nature exposure:
- 20-30 minutes outdoors daily
- Reduces cortisol
- Improves mood
- Natural stress reducer
Adequate recovery:
- Rest days from training
- Vacation time
- Hobbies and enjoyment
- Downtime essential
Social connection:
- Strong relationships
- Regular social interaction
- Reduces stress response
- Support system
What to avoid:
- Overcommitment
- Constant connectivity
- News/social media overload
- Toxic relationships
- Stress amplifiers
Expected improvement:
- Stress management: 50-100 ng/dL increase
- Especially if chronically stressed
- Significant benefit
Strategy 6: Eat Adequate Healthy Fats
Why it’s critical:
- Testosterone synthesized from cholesterol
- Low-fat diets lower testosterone
- Need dietary fat for hormones
- Fat is precursor
The research:
- Diets <20% fat decrease testosterone
- Optimal: 25-35% of calories from fat
- Type of fat matters
- Fat intake crucial
The protocol:
Fat intake:
- 25-30% of total calories from fat
- For 2500 calorie diet: ~70-80g fat daily
- Adequate amount
Fat sources (prioritize):
Saturated fats (yes, really):
- Red meat, butter, coconut oil, eggs
- Direct precursor to testosterone
- 7-10% of calories
- Important for hormones
Monounsaturated fats:
- Olive oil, avocados, nuts
- Anti-inflammatory
- 10-15% of calories
- Heart-healthy
Omega-3 fats:
- Fatty fish (salmon, sardines)
- Fish oil supplement
- Reduces inflammation
- 2-3g EPA+DHA daily
- Anti-inflammatory
Avoid:
- Trans fats (margarine, fried foods)
- Excess omega-6 (vegetable oils)
- Processed fats
- Inflammatory fats
Expected improvement:
- Increasing fat from <20% to 30%: 50-100 ng/dL increase
- Especially if previously low-fat
- Meaningful impact
Strategy 7: Optimize Zinc and Magnesium Intake
Why they matter:
- Both directly involved in testosterone production
- Zinc inhibits aromatase (prevents testosterone → estrogen)
- Magnesium involved in synthesis
- Most people deficient
- Critical minerals
The research:
Zinc:
- Deficiency lowers testosterone significantly
- Supplementation in deficient men increases testosterone 20-30%
- Athletes particularly at risk (lost in sweat)
- Well-documented
Magnesium:
- Increases free and total testosterone
- Especially in exercising individuals
- Most people don’t get enough
- Common deficiency
The protocol:
Zinc:
- 15-30mg daily
- Zinc picolinate or gluconate (better absorption)
- Don’t exceed 40mg long-term (copper imbalance)
- Take with food (upset stomach if empty)
- Daily supplementation
Magnesium:
- 400-500mg daily
- Magnesium glycinate best (absorbable, calming)
- Before bed ideal
- Daily supplementation
Food sources:
- Zinc: Oysters (highest), red meat, poultry, nuts
- Magnesium: Dark leafy greens, nuts, seeds, dark chocolate
- Whole food foundation
Expected improvement:
- If deficient: 50-100 ng/dL increase
- Easy intervention
- Simple fix
Strategy 8: Practice Time-Restricted Eating
Why it works:
- Intermittent fasting increases testosterone
- Growth hormone increases during fasting (supports testosterone)
- Improves insulin sensitivity (insulin-testosterone relationship)
- Hormonal optimization
The research:
- 16:8 time-restricted eating
- Increases testosterone 15-20%
- Preserves muscle if adequate protein
- Moderate fasting beneficial
The protocol:
Time-restricted eating:
- 16-hour fast, 8-hour eating window
- Example: Eat 12 PM – 8 PM, fast 8 PM – 12 PM
- Daily pattern
- Consistent rhythm
Important notes:
- Eat adequate calories in eating window
- High protein (1g+ per pound)
- Lift during eating window (fuel availability)
- Don’t fast longer (excessive fasting lowers testosterone)
- Moderate approach
Who should avoid:
- If chronically stressed (adds stress)
- If underweight (need more calories)
- If training very early morning (need fuel)
- Individual considerations
Expected improvement:
- 50-100 ng/dL increase
- Also improves body composition
- Multiple benefits
Strategy 9: Cold Exposure (Testicular Cooling)
Why it works:
- Testicles produce testosterone optimally at slightly below body temperature
- Overheating impairs production
- Cooling may enhance production
- Temperature matters
The research:
- Chronic heat exposure lowers testosterone
- Cooling may increase production
- Moderate evidence
- Interesting mechanism
The protocol:
Avoid excessive heat:
- No hot tubs/saunas daily
- No laptop on lap
- Loose-fitting underwear (boxers, not briefs)
- Avoid sitting for extended periods
- Reduce heat exposure
Optional cold exposure:
- Cold showers (30-60 seconds cold at end)
- Ice bath post-workout (10-15 minutes)
- May enhance testosterone
- Experimental
Expected improvement:
- Modest effect (20-50 ng/dL)
- More about preventing suppression
- Supportive strategy
The Supplement Protocol (Evidence-Based Only)
What actually works (and what doesn’t).
Tier 1: Strong Evidence (Use These)
Vitamin D3:
- 4000-5000 IU daily (if deficient)
- With vitamin K2 (100-200mcg)
- Non-negotiable if deficient
- Expected increase: 100-200 ng/dL (if deficient)
Zinc:
- 15-30mg daily
- Zinc picolinate or gluconate
- Critical mineral
- Expected increase: 50-100 ng/dL (if deficient)
Magnesium:
- 400-500mg daily
- Magnesium glycinate
- Foundation supplement
- Expected increase: 30-80 ng/dL (if deficient)
Omega-3 fish oil:
- 2-3g EPA+DHA daily
- Reduces inflammation
- Supports overall hormonal health
- Anti-inflammatory
Vitamin K2:
- 100-200mcg daily
- With vitamin D
- Proper calcium regulation
- Supports vitamin D
Tier 2: Moderate Evidence (May Help)
D-Aspartic Acid (DAA):
- 2-3g daily for 1-2 weeks
- May increase testosterone 30-40% in men with low baseline
- Less effective if already normal
- Don’t use continuously (downregulates receptors)
- Short-term boost
Ashwagandha:
- 300-600mg daily (standardized extract)
- Reduces cortisol (allows testosterone to rise)
- Modest testosterone increase (10-15%)
- Stress reduction primary benefit
- Adaptogen
Fenugreek:
- 500mg daily
- May increase free testosterone
- Mixed evidence
- Modest effect
- Possible benefit
Boron:
- 6-10mg daily
- May increase free testosterone
- Reduces SHBG (sex hormone binding globulin)
- Modest effect
- Mineral supplement
Tier 3: Weak Evidence (Save Your Money)
Tribulus terrestris:
- Popular but doesn’t work
- Multiple studies show no effect
- Waste of money
Horny goat weed:
- No evidence for testosterone increase
- Marketing hype
Most “testosterone booster” products:
- Proprietary blends
- Underdosed ingredients
- Expensive
- Little to no evidence
- Save your money
The Complete Supplement Stack
Daily protocol:
Morning:
- Vitamin D3 (4000-5000 IU) + K2 (100-200mcg)
- Omega-3 (2-3g EPA+DHA)
- Zinc (15-30mg)
Evening:
- Magnesium glycinate (400-500mg)
- Ashwagandha (300-600mg) if high stress
Optional cycles:
- D-Aspartic Acid (2-3g for 1-2 weeks every 2-3 months)
Monthly cost:
- ~$40-60 for quality supplements
- Affordable
Expected total improvement:
- From supplements alone: 150-300 ng/dL (if deficient)
- Combined with lifestyle: 300-500+ ng/dL
- Significant impact

When to Consider Medical Intervention
Knowing when natural isn’t enough.
Get Tested First
Essential labs:
Hormone panel:
- Total testosterone (optimal: 700-1000+ ng/dL)
- Free testosterone (optimal: 15-25+ pg/mL)
- SHBG (sex hormone binding globulin)
- Estradiol (should be 20-40 pg/mL)
- LH and FSH (pituitary hormones)
- Complete picture
Supporting labs:
- Vitamin D
- Thyroid (TSH, Free T3, Free T4)
- Prolactin (can suppress testosterone)
- Metabolic panel
- Rule out other issues
When to test:
- Morning (8-10 AM when testosterone peaks)
- Fasted
- Multiple tests (testosterone varies day-to-day)
- Accurate assessment
Scenarios for Medical Treatment
Scenario 1: Truly low testosterone (<300 ng/dL)
- Multiple tests confirm
- Significant symptoms
- Natural methods insufficient
- TRT consideration appropriate
- Medical necessity
Scenario 2: Low-normal with severe symptoms (300-400 ng/dL)
- Quality of life severely affected
- Natural optimization attempted
- Still symptomatic
- Consider medical treatment
- Case-by-case
Scenario 3: Optimal levels but still symptomatic (>500 ng/dL)
- Testosterone not the issue
- Investigate other causes
- Thyroid, sleep apnea, depression, etc.
- Wrong target
TRT (Testosterone Replacement Therapy)
What it is:
- Exogenous testosterone administration
- Injections most common
- Creams/gels alternative
- Medical treatment
When appropriate:
- True hypogonadism (<300 ng/dL)
- Quality of life severely impacted
- Natural methods tried and failed
- Under physician supervision
- Last resort
Important considerations:
Pros:
- Reliably increases testosterone to high-normal
- Improves symptoms
- Better quality of life
- Effective treatment
Cons:
- Shuts down natural production
- Lifelong commitment
- Fertility issues (suppresses sperm production)
- Potential side effects (cardiovascular, prostate)
- Regular monitoring required
- Serious decision
The approach:
- Try natural optimization first (6-12 months)
- If insufficient, consult endocrinologist
- Comprehensive evaluation
- Informed decision
- Medical guidance essential
The Complete Testosterone Optimization Protocol
Putting it all together.
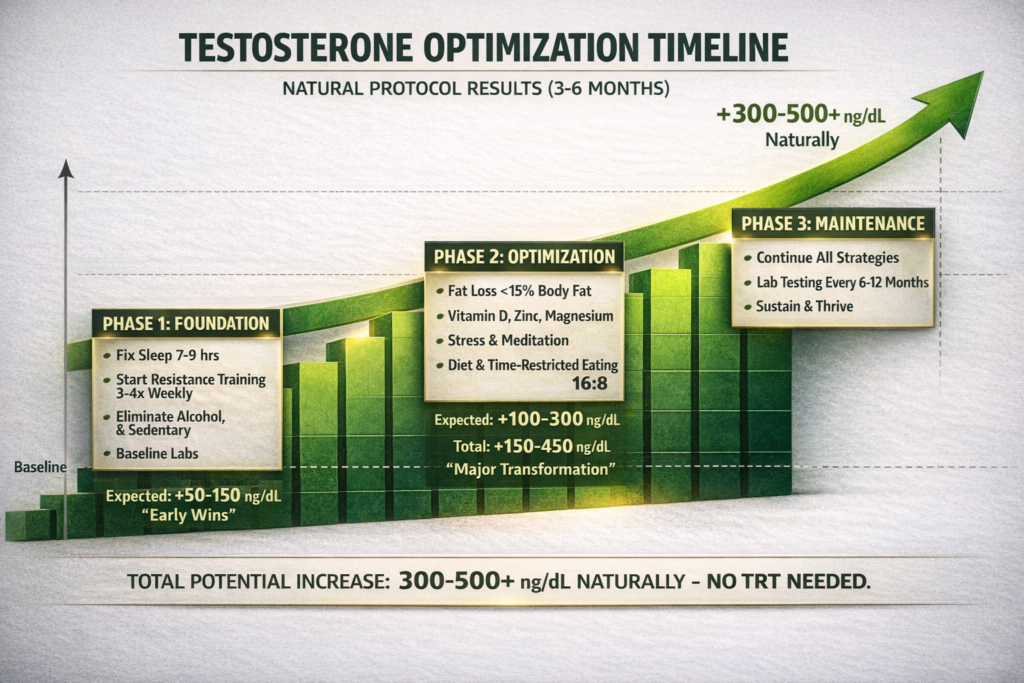
Phase 1: Foundation (Weeks 1-4)
Priority actions:
- Get comprehensive lab work (baseline)
- Fix sleep (7-9 hours nightly, consistent schedule)
- Start resistance training (3-4x weekly)
- Eliminate obvious testosterone killers (excess alcohol, poor sleep, sedentary)
- Build foundation
Expected improvement:
- 50-150 ng/dL increase
- Noticeable energy improvement
- Early wins
Phase 2: Optimization (Weeks 5-12)
Add:
- Fat loss protocol (if overweight, target <15% body fat)
- Supplement protocol (vitamin D, zinc, magnesium, omega-3)
- Stress management practices (meditation, breathing)
- Dietary optimization (adequate fats, whole foods)
- Time-restricted eating (16:8)
- Full optimization
Expected improvement:
- Additional 100-300 ng/dL increase
- Total improvement: 150-450 ng/dL from baseline
- Significant physique changes
- Major transformation
Phase 3: Maintenance (Week 13+)
Continue:
- All strategies from Phase 1-2
- Regular lab testing (every 6-12 months)
- Consistent lifestyle
- Sustain results
Monitor:
- Energy levels
- Body composition
- Strength and performance
- Libido
- Mood
- Track progress
Sample Day of Testosterone-Optimized Living
Example for 180lb man:
Morning (7:00 AM):
- Wake naturally (7-9 hours sleep)
- 10-20 minutes morning sunlight
- Cold shower (optional, 30-60 seconds cold)
- Start day right
Breakfast (8:00 AM):
- 4 whole eggs, scrambled
- 2 slices turkey bacon
- Avocado
- Spinach
- High protein, healthy fats, testosterone-supporting
Supplements (with breakfast):
- Vitamin D3 (5000 IU) + K2 (200mcg)
- Zinc (30mg)
- Omega-3 (3g)
- Morning stack
Mid-morning (10:30 AM):
- Black coffee (optional)
- Walk outside 10-15 minutes
- Activity and sunlight
Lunch (12:30 PM):
- 8oz steak
- Sweet potato
- Broccoli
- Olive oil dressing
- Protein and healthy carbs
Afternoon (3:00 PM):
- Brief walk
- Stress management (10-minute meditation or breathing)
- Cortisol control
Pre-workout (4:00 PM):
- 1 banana
- Black coffee
- Fuel for training
Training (5:00 PM):
- Resistance training session
- Squats, bench press, rows, overhead press
- 45-60 minutes
- Progressive overload
- Testosterone-boosting workout
Dinner (7:00 PM):
- 8oz salmon
- Quinoa
- Asparagus
- Nuts and seeds
- Anti-inflammatory, nutrient-dense
Evening supplement (9:00 PM):
- Magnesium glycinate (400mg)
- Ashwagandha (if high stress, 600mg)
- Evening stack
Wind down (9:30 PM):
- No screens
- Dim lights
- Cool room (65-68°F)
- Reading or light stretching
- Sleep preparation
Bed (10:00 PM):
- 8-9 hours sleep
- Dark, cool room
- Consistent schedule
- Recovery and testosterone production
Daily totals:
- Protein: 200g (1.1g per pound)
- Fat: 90g (30% of calories)
- Carbs: 200g (strategically timed)
- Calories: ~2400
- Testosterone-optimized nutrition
The Bottom Line: Optimize Testosterone Naturally
After explaining everything:
The truth about testosterone optimization:
✅ Most men can increase testosterone 300-500 ng/dL naturally (no TRT needed)
✅ Lifestyle factors more powerful than supplements (fix sleep, training, body fat first)
✅ The difference between 300 and 800 ng/dL is life-changing (energy, physique, mood, performance)
✅ Takes 3-6 months to see full results (but improvements start immediately)
✅ Sustainable long-term (unlike TRT, maintains natural production)
Key takeaways:
Why testosterone matters:
- Builds muscle and burns fat
- Improves energy and mood
- Enhances sexual function
- Supports metabolic health
- Determines response to training
- Master hormone
What’s destroying your testosterone:
- Obesity and body fat (aromatase converts testosterone to estrogen)
- Poor sleep (<7 hours) (testosterone produced during sleep)
- Chronic stress (cortisol suppresses testosterone)
- Sedentary lifestyle (inactivity allows decline)
- Poor diet (insufficient fats, calories)
- Environmental toxins (xenoestrogens)
- Excess alcohol (direct toxicity)
- Certain medications (opioids, statins, SSRIs)
- Modern life is testosterone killer
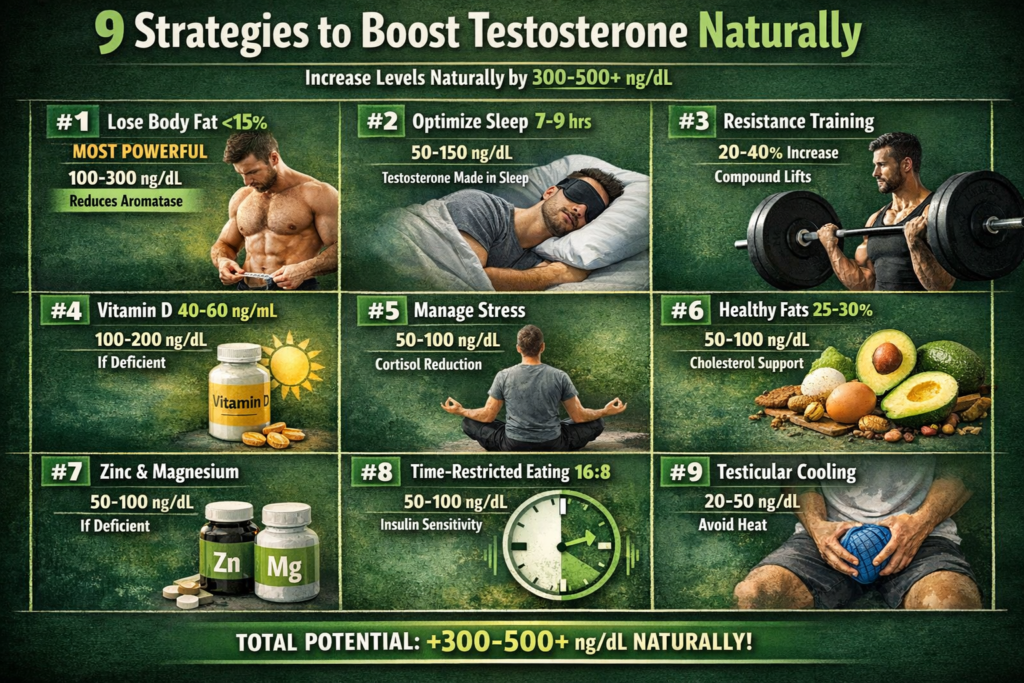
The 9 natural strategies:
- Lose excess body fat (<15% optimal) – Most powerful, 100-300 ng/dL increase
- Optimize sleep (7-9 hours) – Essential, 50-150 ng/dL increase
- Resistance training (progressive overload) – Acute and chronic benefits, 20-40% increase
- Optimize vitamin D (40-60 ng/mL) – If deficient, 100-200 ng/dL increase
- Manage stress (meditation, breathing, nature) – 50-100 ng/dL increase
- Adequate healthy fats (25-30% calories) – 50-100 ng/dL increase
- Zinc and magnesium (daily supplementation) – If deficient, 50-100 ng/dL increase
- Time-restricted eating (16:8) – 50-100 ng/dL increase
- Testicular cooling (avoid excessive heat) – 20-50 ng/dL increase
- Complete protocol
The supplement protocol:
- Vitamin D3 (5000 IU) + K2 (200mcg) daily
- Zinc (30mg) daily
- Magnesium glycinate (400mg) daily
- Omega-3 (2-3g EPA+DHA) daily
- Ashwagandha (600mg) if stressed
- D-Aspartic Acid (short cycles)
- Evidence-based only
What doesn’t work:
- Tribulus terrestris (no evidence)
- Most “testosterone booster” products (proprietary blends, underdosed)
- Horny goat weed (marketing hype)
- Save your money
When to consider TRT:
- Total testosterone <300 ng/dL (multiple tests)
- Natural optimization tried for 6-12 months
- Severe symptoms affecting quality of life
- Under endocrinologist supervision
- Last resort
The timeline:
- Week 1-4: Foundation (sleep, training) – 50-150 ng/dL increase
- Week 5-12: Full optimization (all strategies) – Additional 100-300 ng/dL
- Total potential increase: 300-500+ ng/dL naturally
- Improvements start immediately but full results take 3-6 months
- Patience and consistency
Priority hierarchy:
- Fix sleep (7-9 hours) – Most critical
- Lose body fat (<15%) – Most powerful
- Resistance training (3-4x weekly) – Essential
- Supplement deficiencies (vitamin D, zinc, magnesium) – Easy wins
- Manage stress (daily practices) – Important
- Optimize diet (fats, calories) – Foundation
- Time-restricted eating (16:8) – Supportive
- Start with highest impact
MOST MEN CAN RESTORE TESTOSTERONE TO OPTIMAL LEVELS NATURALLY. NO TRT NEEDED. JUST SCIENCE-BASED LIFESTYLE OPTIMIZATION.
Ready to build a complete testosterone optimization system with proper lab testing, progressive training protocols, strategic nutrition timing, supplement guidance, and lifestyle strategies that restore your hormonal health, transform your physique, and give you the energy and drive you had in your 20s? Understanding testosterone is just the beginning. Get a comprehensive guide to implementing every strategy correctly, tracking progress objectively, troubleshooting plateaus, and achieving optimal testosterone levels that last. Stop accepting low testosterone as “normal aging.” Start optimizing your hormones naturally for peak performance.
REFERENCES
SECTION 1 — Testosterone Decline in Modern Men
[1] Travison TG et al. — Journal of Clinical Endocrinology & Metabolism, 2007 A population-level decline in serum testosterone levels in American men — population-level analysis of 1,532 men across three cohorts (1987–2004); mean testosterone declined ~1.2% per year independent of age; 60-year-old man in 2004 had testosterone ~17% lower than 60-year-old in 1987; decline not explained by BMI, smoking, or health status alone https://pubmed.ncbi.nlm.nih.gov/17062768/
[2] Andersson AM et al. — Journal of Clinical Endocrinology & Metabolism, 2007 Secular decline in male testosterone and sex hormone binding globulin serum levels in Danish population surveys — Danish population cohort study; total testosterone levels fell significantly between 1980s and 2000s; concurrent rise in SHBG reducing free testosterone further; environmental and lifestyle factors implicated https://pubmed.ncbi.nlm.nih.gov/17062764/
SECTION 2 — Obesity, Body Fat, and Aromatase
[3] Zumoff B et al. — Metabolism, 1990 Plasma free and non-sex-hormone-binding-globulin-bound testosterone are decreased in obese men in proportion to their degree of obesity — testosterone inversely correlated with BMI and body fat percentage; free testosterone suppressed by elevated SHBG and aromatization; visceral fat identified as primary driver; weight loss of 10% associated with significant testosterone recovery https://pubmed.ncbi.nlm.nih.gov/2314400/
[4] Grossmann M — Clinical Endocrinology, 2011 Low testosterone in men with type 2 diabetes: significance and treatment — obesity-driven aromatase overexpression converts testosterone to estradiol; hyperinsulinemia suppresses LH pulsatility; each 4-unit BMI increase associated with ~75 ng/dL testosterone reduction; fat loss primary intervention for testosterone restoration in overweight men https://pubmed.ncbi.nlm.nih.gov/21138454/
SECTION 3 — Sleep and Testosterone Production
[5] Leproult R & Van Cauter E — JAMA, 2011 Effect of 1 week of sleep restriction on testosterone levels in young healthy men — 10 healthy young men; sleep restricted to 5 hours/night for 1 week; daytime testosterone levels decreased 10–15%; decline equivalent to 10–15 years of aging; testosterone levels lowest in afternoon (2–10 PM) during restriction period https://pubmed.ncbi.nlm.nih.gov/21632481/
[6] Andersen ML & Tufik S — Hormones and Behavior, 2008 The effects of testosterone on sleep and sleep-disordered breathing in men — bidirectional relationship between testosterone and sleep quality; REM sleep critical for pulsatile LH release and subsequent testosterone synthesis; sleep apnea significantly reduces testosterone via sleep architecture disruption; treatment of apnea restores testosterone levels https://pubmed.ncbi.nlm.nih.gov/18573486/
SECTION 4 — Resistance Training and Testosterone
[7] Kraemer WJ & Ratamess NA — Endocrinology and Metabolism Clinics of North America, 2005 Hormonal responses and adaptations to resistance exercise and training — acute testosterone elevation 15–25% following heavy compound resistance exercise; magnitude proportional to muscle mass recruited, intensity (70–85% 1RM), and rest interval length; chronic resistance training maintains higher baseline testosterone; overtraining reverses these gains https://pubmed.ncbi.nlm.nih.gov/15863128/
[8] Häkkinen K et al. — European Journal of Applied Physiology, 2001 Basal concentrations and acute responses of serum hormones and strength development during heavy resistance training in middle-aged and elderly men and women — progressive resistance training over 6 months significantly elevated resting testosterone; compound multi-joint exercises (squat, deadlift) produced greatest hormonal response; 3–4 sessions/week optimal stimulus https://pubmed.ncbi.nlm.nih.gov/11374102/
SECTION 5 — Vitamin D and Testosterone
[9] Pilz S et al. — Hormone and Metabolic Research, 2011 Effect of vitamin D supplementation on testosterone levels in men — 165 men randomized to 3,332 IU vitamin D daily vs. placebo for 12 months; vitamin D group increased total testosterone from 10.7 to 13.4 nmol/L (+25%); free and bioavailable testosterone also increased significantly; placebo group showed no change; vitamin D receptors identified in testicular Leydig cells https://pubmed.ncbi.nlm.nih.gov/21154195/
SECTION 6 — Cortisol, Stress, and Testosterone Suppression
[10] Cumming DC et al. — Journal of Clinical Endocrinology & Metabolism, 1983 Acute suppression of testosterone by cortisol in men — exogenous cortisol administration acutely suppressed LH pulsatility and testosterone synthesis; cortisol inhibits Leydig cell steroidogenesis at multiple enzymatic steps; chronic psychological stress maintains elevated cortisol with sustained testosterone suppression https://pubmed.ncbi.nlm.nih.gov/6300395/
[11] Lopresti AL et al. — Medicine, 2019 A randomized, double-blind, placebo-controlled, crossover study examining the hormonal and vitality effects of ashwagandha in aging, overweight males — 57 men, 300mg ashwagandha extract twice daily for 8 weeks; testosterone increased 14.7% vs. placebo; DHEA-S increased 18%; salivary cortisol significantly reduced; mechanism via HPA axis modulation and cortisol reduction https://pubmed.ncbi.nlm.nih.gov/31672867/
SECTION 7 — Dietary Fat and Testosterone
[12] Hamalainen E et al. — Hormone Research, 1984 Diet and serum sex hormone levels — controlled dietary intervention manipulating fat and fiber intake; shift from high-fat (40%) to low-fat (25%) diet significantly reduced total and free testosterone; saturated fat and monounsaturated fat intake positively correlated with testosterone; dietary fat provides cholesterol substrate for steroidogenesis https://pubmed.ncbi.nlm.nih.gov/6538617/
[13] Volek JS et al. — Journal of Applied Physiology, 1997 Testosterone and cortisol in relationship to dietary nutrients and resistance exercise — 12 experienced resistance-trained men; dietary fat intake significantly positively correlated with resting testosterone; protein-to-carbohydrate ratio and fat intake predicted testosterone response to resistance exercise; saturated and monounsaturated fats most strongly correlated https://pubmed.ncbi.nlm.nih.gov/9139178/
SECTION 8 — Zinc, Magnesium, and Testosterone
[14] Prasad AS et al. — Nutrition, 1996 Zinc status and serum testosterone levels of healthy adults — zinc-restricted diet for 20 weeks reduced testosterone from 39.9 to 10.6 nmol/L in young men; zinc supplementation in elderly deficient men doubled testosterone from 8.3 to 16.0 nmol/L; zinc inhibits aromatase enzyme activity; athletes particularly vulnerable due to zinc losses in sweat https://pubmed.ncbi.nlm.nih.gov/8875519/
[15] Cinar V et al. — Biological Trace Element Research, 2011 Effects of magnesium supplementation on testosterone levels of athletes and sedentary subjects at rest and after exhaustion — 4 weeks magnesium supplementation (10mg/kg/day); free and total testosterone increased in both sedentary and athletic groups; greatest effect in exercising individuals; magnesium involved in testosterone synthesis and reduces SHBG binding https://pubmed.ncbi.nlm.nih.gov/20352370/
SECTION 9 — Intermittent Fasting and Testosterone
[16] Röjdmark S et al. — Metabolism, 1989 Pulsatile secretion of gonadotropins during fasting in normal men — short-term fasting increased LH pulse frequency and amplitude; enhanced LH pulsatility drives increased testicular testosterone production; growth hormone also elevated during fasting; effect most pronounced in 16–24 hour fasting windows; prolonged starvation reverses effects https://pubmed.ncbi.nlm.nih.gov/2491498/
SECTION 10 — Environmental Endocrine Disruptors
[17] Gore AC et al. — Endocrine Society Scientific Statement, 2015 EDC-2: The Endocrine Society’s second scientific statement on endocrine-disrupting chemicals — comprehensive review of xenoestrogen mechanisms; BPA, phthalates, and parabens bind estrogen receptors and suppress androgen signaling; prenatal and adult exposure suppresses testosterone production; cumulative daily exposure from plastics, personal care products, and pesticides https://pubmed.ncbi.nlm.nih.gov/26544531/
SECTION 11 — Alcohol and Testosterone
[18] Välimäki MJ et al. — Journal of Steroid Biochemistry, 1984 The pulsatile secretion of gonadotropins and growth hormone, and the biological activity of luteinizing hormone in men acutely intoxicated with ethanol — acute alcohol intake suppressed testosterone within 30 minutes via direct Leydig cell toxicity; LH pulsatility disrupted; testosterone suppression lasted 24–48 hours post-binge episode; chronic alcoholism causes sustained hypogonadism and testicular atrophy https://pubmed.ncbi.nlm.nih.gov/6540786/






Leave a Reply
You must be logged in to post a comment.